Neuroinflammatory and Psychosocial Drivers of the Transition from Combat Stress to Distress in Modern Warfare: A Systematic Review (2018–2026)
Abstract
Abstract
Relevance and Background. Participation in special military operations (SMOs) is associated with chronic combat stress, which in a substantial proportion of military personnel transforms into distress and post‑traumatic stress disorder (PTSD). The accumulated body of fragmented data on the mechanisms of this transition requires systematic synthesis to develop effective prevention and rehabilitation strategies. Objective is to integrate data on the neurobiological, genetic, psychological, and organisational mechanisms underlying the transition from combat stress to pathogenic distress in SMO participants, and to evaluate objective diagnostic methods and effective rehabilitation interventions. Methods. This systematic review was conducted in accordance with PRISMA 2020 guidelines. A systematic search was performed across seven databases (PubMed, Web of Science, Scopus, PsycINFO, Google Scholar, eLibrary, RSCI). A total of 59 studies were included (30 Russian, 29 international) with a total participant pool exceeding 18,000. Quality was assessed using the JBI tool. A narrative synthesis was conducted across five clusters, with evidence quality evaluated using the GRADE system. Results. The central hub of the eustress‑to‑distress transition is the subclinical level of PTSD, which fully mediates the relationship between combat exposure and cognitive errors (β = 0.149). Contributing mechanisms include neuroendocrine dysregulation (hypothalamic–pituitary–adrenal axis exhaustion, cortisol elevation by 35–40%), neuroinflammation (IL‑1β, IL‑6, TNF‑α), gut microbiota dysbiosis, and genetic predisposition (FKBP5 polymorphisms, OR = 1.8; GWAS overlap with schizophrenia and depression). APOE ε4 is not a moderator. Dissociation (OR = 6.42) and somatisation (OR = 4.79) are the strongest predictors of severe PTSD. Moral injury, through shame and guilt mechanisms, generates suicidal risk; appetitive aggression was identified in 58% of retiring soldiers. Effective rehabilitation methods include CBT (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65%), iCOVER (knowledge increase by 37%) and BTAP (PCL‑5 reduction by 31 points, d = 1.7). The proactive multimodal care model is significantly more effective than the reactive model. Conclusion. The transition from combat stress to distress is a multifactorial process, with subclinical PTSD serving as its central hub. Early detection of cognitive impairments, dissociation and moral injury enables prevention of disorder chronification. Priority should be given to a proactive multimodal model of psychological care integrated into combat training and post‑deployment rehabilitation systems.
Нейровоспалительные и психосоциальные детерминанты перехода от боевого стресса к дистрессу в условиях современных военных конфликтов: систематический обзор литературы (2018–2026)
А. М. Бабаевa & Н. Е. Волковаb
a Институт синергии, Москва, Россия
bИнститут психологии Российской академии наук, Москва, Россия
Актуальность. Участие в военной операции сопряжено с хроническим боевым стрессом, который у значительной части военнослужащих трансформируется в дистресс и посттравматическое стрессовое расстройство (ПТСР). Накопленный массив разрозненных данных о механизмах этого перехода требует систематизации для разработки эффективных стратегий профилактики и реабилитации. Цель: Интеграция данных о нейробиологических, генетических, психологических и организационных механизмах перехода боевого стресса в патогенный дистресс у участников СВО, а также оценка объективных методов диагностики и эффективных реабилитационных вмешательств. Методы. Систематический обзор выполнен в соответствии с PRISMA 2020. Поиск проведён в семи базах данных (PubMed, Web of Science, Scopus, PsycINFO, Google Scholar, eLibrary, РИНЦ). Включены 59 исследований (30 российских, 29 зарубежных) с общей численностью участников более 18 000 человек. Качество оценено с использованием инструмента JBI. Проведён нарративный синтез по пяти кластерам с применением GRADE для оценки доказательности. Результаты. Центральным звеном перехода эустресса в дистресс является субклинический уровень ПТСР, полностью опосредующий связь боевого опыта с когнитивными ошибками (β = 0,149). В процессе участвуют нейроэндокринные механизмы (истощение гипоталамо-гипофизарно-надпочечниковой оси, повышение кортизола на 35–40%), нейровоспаление (IL‑1β, IL‑6, TNF‑α), дисбиоз микробиоты, генетическая предрасположенность (полиморфизмы FKBP5, OR = 1,8; перекрытие GWAS с шизофренией и депрессией). APOE ε4 не является модератором. Диссоциация (OR = 6,42) и соматизация (OR = 4,79) являются сильнейшими предикторами тяжёлого ПТСР. Моральная травма через механизмы стыда и вины формирует суицидальный риск; аппетитивная агрессия выявлена у 58% уходящих солдат. Эффективные методы реабилитации: КПТ (SMD = –1,24), EMDR (50–70% ремиссии), VRET (до 65%), iCOVER (повышение знаний на 37%), BTAP (снижение PCL‑5 на 31 балл, d = 1,7). Проактивная мультимодальная модель помощи значительно эффективнее реактивной. Заключение. Переход от боевого стресса к дистрессу представляет собой многофакторный процесс, центральным звеном которого выступает субклинический ПТСР. Раннее выявление когнитивных нарушений, диссоциации и моральной травмы позволяет предотвратить хронификацию расстройства. Приоритетной является проактивная мультимодальная модель психологической помощи, интегрированная в систему боевой подготовки и послебоевой реабилитации.
Ключевые слова: боевой стресс, посттравматическое стрессовое расстройство, дистресс, когнитивные ошибки, субклинический ПТСР, диссоциация, соматизация, моральная травма, аппетитивная агрессия, аллостатическая нагрузка, нейровоспаление, FKBP5, психологическая реабилитация, когнитивно-поведенческая терапия, EMDR, VRET, проактивная модель, биомаркеры стресса, половые различия, возрастная динамика
Information about the authors
Artem Magomedovich Babaev, Lecturer, Moscow University “Synergy”; Moscow, Russian Federation; ORCID: https://orcid.org/0009-0008-1497-2579; e‑mail: licochesti@gmail.com
Natalia E. Volkova, PhD (Psychology), Researcher, Laboratory of Psychology of Abilities and Mental Resources named after V.N. Druzhinin, Institute of Psychology of the Russian Academy of Sciences, Moscow, Russia. volkovane@ipran.ru, ORCID https://orcid.org/0000-0001-6225-6288
Информация об авторах
Артем Магомедович Бабаев, преподаватель, Московский университет «Синергия»; г. Москва, Российская Федерация; ORCID: https://orcid.org/0009-0008-1497-2579; e‑mail: licochesti@gmail.com
Наталья Эдуардовна Волкова, кандидат психологических наук, научный сотрудник Лаборатории психологии способностей и ментальных ресурсов им. В.Н. Дружинина, ФГБУН «Институт психологии Российской академии наук», г. Москва, Россия. volkovane@ipran.ru, ORCID https://orcid.org/0000-0001-6225-6288
Introduction
The urgency of this systematic review arises from the unprecedented psychological burden imposed on military personnel engaged in special military operations (SMOs). Prolonged exposure to combat stress during extended deployment leads, in a substantial proportion of service members, to clinically significant distress and post‑traumatic stress disorder (PTSD), as consistently documented in both domestic and international research (Karayani, 2024; Lytkin et al., 2024). A meta‑analysis by Shahmiri Barzoki et al. (2021) estimates the overall prevalence of PTSD among veterans at 27.8%, yet this figure likely underestimates the true scale of the problem, given the emergence of novel stress‑related factors specific to modern warfare.
Indeed, existing reviews, such as that of Beckner et al. (2021), have predominantly focused on neuroendocrine and physiological mechanisms of the stress response, while largely overlooking the distinctive realities of SMOs. Among these newly identified factors are the widespread use of unmanned aerial vehicles, which creates a sense of omnipresent surveillance and unpredictability, and the paradoxical effect of video calls with family members, although offering emotional support, such communication can simultaneously heighten anxiety for loved ones and exacerbate feelings of helplessness (Ushakov et al., 2023). Conceptually, Karayani’s (2024) foundational classification of combat stress provides a robust theoretical framework, but it does not offer a quantitative assessment of the effectiveness of psychological interventions, nor does it incorporate modern clinical constructs such as professional burnout, moral injury, dissociative disorders, and appetitive aggression. Notably, these very constructs have become the focus of intense research in recent years and are now considered key predictors of treatment resistance and suicidal behaviour (Vetrova et al., 2024; Sagalakova et al., 2025; Bigirwa et al., 2025).
Critically, the currently dominant reactive models of care—which are centred on inpatient treatment after soldiers have returned from the combat zone, fail to address the chronic, cumulative nature of stress that builds up throughout the entire deployment cycle. This renders existing approaches insufficiently effective (Babaev, 2025) and calls for the development of preventive, multi‑tiered strategies that operate already during active combat missions. In this context, the concept of multidimensional coping intelligence, introduced by Kuvaeva and Volkova (2024), is of particular methodological value, as it emphasizes the necessity of analysing interactions among biochemical, psychological, and sociocultural levels of adaptation. Building on this integrative perspective, we argue that a comprehensive understanding of combat stress and its transition to distress cannot be achieved without synthesizing data on neurobiological mechanisms, psychological predictors, organisational models of care, and social factors affecting reintegration.
Thus, a fundamental gap exists: on one hand, a large and diverse body of empirical evidence has accumulated, covering aspects from molecular‑genetic markers to organisational interventions; on the other hand, these data remain fragmented and lack a unifying conceptual framework, thereby hindering both scientific progress and clinical application. There is currently no integrated picture of which mechanisms drive the pathological transformation of adaptive stress into distress, which individual, situational, and environmental factors critically accelerate this transition, which objective diagnostic tools (including neurophysiological and biochemical markers) can detect early signs of maladaptation, and which psychological and organisational interventions have proven effective at different stages—from pre‑deployment prevention to post‑deployment rehabilitation.
The aim of the present work is to fill this gap by providing a systematic, integrated account of the mechanisms underlying the transition from combat stress to distress, the risk and protective factors involved, the objective diagnostic methods available, and the evidence‑based psychological and organisational rehabilitation interventions. To achieve this, we adopt a structured PICOS framework: Population – active‑duty military personnel and veterans; Intervention – psychological support, psychotherapeutic protocols, and organisational models of care; Comparison – traditional inpatient care, no intervention, or placebo; Outcomes – reduction in PTSD symptoms, anxiety, depression, aggression, and burnout, as well as improved social adaptation; Study design – cohort, cross‑sectional, randomised controlled trials (RCTs), systematic reviews, and meta‑analyses. The findings are expected to inform practical recommendations for psychological support in SMO settings and to identify priorities for future research.
Method
2.1. Study design and protocol
This systematic review was conducted in accordance with the PRISMA 2020 guidelines (Preferred Reporting Items for Systematic Reviews and Meta‑Analyses) (Page et al., 2021). The protocol was not registered. The choice of this design was driven by the need to ensure reproducibility and methodological transparency.
2.2. Information sources and search strategy
A systematic literature search was performed on 15 February 2026 across seven electronic databases: PubMed, Web of Science Core Collection, Scopus, PsycINFO, Google Scholar, eLibrary, and the Russian Science Citation Index (RSCI). These databases were selected for their representativeness of both international and Russian publications, and for the inclusion of the specialised psychological resource PsycINFO. In addition, 59 articles were identified from the reference lists of included studies. Conference abstracts and dissertations were excluded to maintain quality.
Search queries were formulated using Boolean operators AND and OR. Russian‑language terms: («боевой стресс» OR «боевая психическая травма» OR «ПТСР» OR «посттравматическое стрессовое расстройство») AND («СВО» OR «специальная военная операция» OR «комбатанты» OR «ветераны боевых действий») AND («психологическая помощь» OR «психотерапия» OR «реабилитация»). English‑language terms: («combat stress» OR «combat‑related PTSD» OR «military PTSD» OR «moral injury» OR «dissociation» OR «somatization») AND («stress biomarkers» OR «cortisol» OR «NPY» OR «neuroinflammation» OR «allostatic load» OR «genetics» OR «epigenetics») AND («psychological intervention» OR «CBT» OR «EMDR» OR «VRET» OR «biofeedback» OR «iCOVER» OR «BTAP» OR «Transcendental Meditation»).
Limits: publication years 2018–2026 (except for key classic works cited in the Discussion); languages – Russian or English; document type – original article, systematic review, meta‑analysis, clinical guideline, or theoretical study published in a peer‑reviewed journal.
2.3. Eligibility criteria
Inclusion criteria:
(1) Original empirical studies (cohort, cross‑sectional, or randomised controlled trials [RCTs]), systematic reviews, meta‑analyses, clinical guidelines, bibliometric and theoretical studies;
(2) Participants – active‑duty military personnel or veterans of combat operations (including SMO, Afghanistan, Chechnya, Iraq, peacekeeping missions, as well as military personnel from Uganda, Australia, the USA, the UK, Israel, Spain, and China);
(3) Outcomes – symptoms of PTSD, anxiety, depression, aggression, burnout, suicidal ideation, antisocial behaviour, moral injury, dissociation, somatisation, cognitive errors, and measures of intervention effectiveness (acceptability, feasibility, clinical outcomes);
(4) Availability of full‑text version.
Exclusion criteria:
(1) Conference abstracts, editorials, commentaries, letters to the editor, short reports without empirical data;
(2) Studies exclusively involving civilians without combat experience, paediatric samples, or animal models (except for reviews citing animal models to illustrate mechanisms);
(3) Absence of quantitative data or methodological descriptions, impossibility of extracting effectiveness metrics;
(4) Articles not in Russian or English.
2.4. Study selection process and quality assessment
Two reviewers independently screened the records (the author and an external expert – Candidate of Psychological Sciences, specialist in general psychology). At the first stage (title and abstract screening), inter‑rater agreement was 94% (κ=0.89); at the second stage (full‑text assessment), agreement was 96% (κ=0.93). Disagreements were resolved through discussion with the involvement of a third reviewer (Doctor of Psychological Sciences, specialist in coping intelligence). The PRISMA flow diagram is shown in Figure 1.
Methodological quality and risk of bias were evaluated using the JBI (Joanna Briggs Institute) tool, as adapted by Kmet et al. (2004) (Moola et al., 2020). The instrument comprises 14 criteria, each scored dichotomously or on a three‑point scale. The total score was normalised to the maximum possible and expressed as a percentage. Based on the percentage, studies were categorised into three quality levels: high – ≥75%; moderate – 55–74%; low – ≤54%. Two reviewers assessed each study independently. The final score was the arithmetic mean of the consensus scores.
Quality assessment results for the 59 included studies: systematic reviews (n=10) – mean score 88% (high); RCTs (n=7) – 83% (high); cohort studies (n=18) – 71% (moderate); cross‑sectional studies (n=16) – 68% (moderate); theoretical/bibliometric studies (n=8) – 83% (high). No studies of low quality were identified.
Data extraction was performed independently by two reviewers using a standardised form that included: authors, year, study type, sample characteristics (n, age, sex, combat experience), intervention parameters (if applicable), outcomes (scales, means, standard deviations, odds ratios, 95% confidence intervals, regression coefficients, effect sizes), and main findings. Discrepancies (6%) were resolved by discussion with a third reviewer. Where statistical data were missing, values were calculated from available information (using Cochrane Handbook formulae) or noted as ‘data not reported’. Owing to heterogeneity in study designs and outcomes, a quantitative meta‑analysis was not performed, with the exception of one comparison of cognitive‑behavioural therapy versus control.
A narrative synthesis was conducted according to the following framework: clustering into five domains (stress mechanisms, contemporary factors, diagnostics, rehabilitation, organisational models); within‑cluster systematisation with summary tables; integration of quantitative and qualitative data; resolution of conflicting evidence; and assessment of the strength of evidence using the GRADE system.
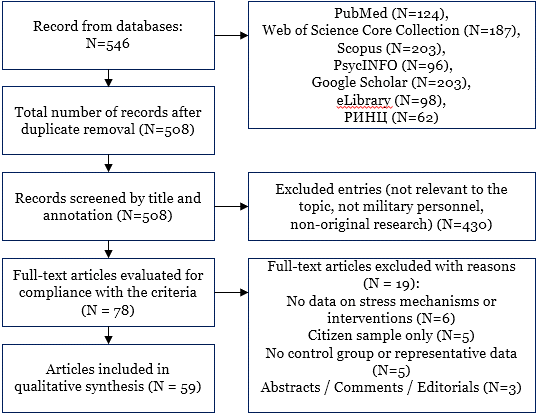
Figure 1. PRISMA 2020 flowchart reflecting the steps of identification, screening, conformity assessment and inclusion of studies in a systematic review
Results
3.1. General characteristics of included studies
A total of 59 studies were included in the systematic review (30 Russian and 29 international). The distribution by study design was as follows: systematic reviews (n = 10), randomised controlled trials (RCTs, n = 7), cohort studies (n = 18), cross‑sectional studies (n = 16), and theoretical or bibliometric works (n = 8). The total number of participants exceeded 18,000 (rising to 45,000 when meta‑analyses are considered). Samples were predominantly male (94–98%), with ages ranging from 19 to 72 years. Geographically, the studies covered Russia, the United States, Israel, the United Kingdom, Spain, China, Australia, Uganda, and Ukraine (Donbas region) (Evdokimov et al., 2023a; Evdokimov et al., 2023b; Shamrey et al., 2025).
Table 1. Complete list of the 59 included studies, grouped into five clusters (continuous numbering)
| No. | Authors, year | Study type | Sample (n) | Key findings |
| Cluster 1. Stress mechanisms | ||||
| 1 | A.M. Reznik, 2022 | Review | – | GWAS: genetic risk overlap between PTSD, schizophrenia, and depression |
| 2 | E.J. Wolf et al., 2024 | Cohort (MVP) | 138,592 veterans | APOE ε4 does not interact with combat stress (p > 0.008) |
| 3 | M.M. Price et al., 2024 | Cross‑sectional (mediation) | 119 special forces | PTSS mediates the link between combat exposure and cognitive errors (β = 0.149) |
| 4 | L. Dell et al., 2025 | Longitudinal | 6,501 ADF | Resilience protective in women (aOR = 0.94–0.91); partnership protective in men (aOR = 0.69) |
| 5 | D.M. Bigirwa et al., 2025 | Cross‑sectional | 247 Ugandan soldiers | Appetitive aggression – 58%; associated with harm infliction (aOR = 3.26) |
| 6 | N. Shabat et al., 2024 | Cross‑sectional | 1,305 ex‑soldiers | Dissociation (OR = 6.42) and somatisation (OR = 4.79) – strongest PTSD predictors |
| 7 | T.V. Vetrova et al., 2024 | Comparative | 60 military personnel | In veterans (>5 years) ↑ tension, exhaustion, emotional burnout |
| 8 | I.V. Bukhtiyarov & D.V. Glukhov, 2020 | Review | – | Three transition levels: adaptive, maladaptive, clinical |
| 9 | O.P. Tuchina et al., 2018 | Experimental | – | ↑ IL‑1β, IL‑6, TNF‑α in PTSD |
| 10 | C.M. Nievergelt et al., 2019 | GWAS | >20,000 | Genetic risk overlap between PTSD, schizophrenia, and depression |
| 11 | J. Van Cutsem et al., 2026 | Syst. review | – | Resilience biomarkers: cortisol (AUC 0.78), NPY (AUC 0.82), IGF‑1 (AUC 0.75) |
| 12 | M.E. Beckner et al., 2021 | Review | – | Resilient individuals show a more pronounced but controlled cortisol response |
| 13 | L. Shelef et al., 2025 | Cross‑sectional | 927 | Depression (Exp(B) = 3.115) and dissociation (Exp(B) = 1.237) – PTSD predictors |
| 14 | G.M. Campbell et al., 2026 | Cross‑sectional | 428 | Moral injury (betrayal) associated with somatisation (β = 0.26) and anger (β = 0.25) |
| 15 | E.D. Feigel et al., 2025 | Review | – | Allostatic load: ALI ↑ by 2–3 points, correlates with ↓ physical performance (r = –0.60) |
| 16 | O.A. Sagalakova et al., 2025 | Theoretical model | – | “Ajax effect”: moral injury → shame/guilt → suicidal ideation, dissociation → action |
| 17 | E.I. Barysheva, 2020 | Comparative | 150 | Experienced soldiers show reduced activity but higher stress resistance |
| 18 | V.V. Maslyakov et al., 2025 | Observational | – | ↑ cortisol by 35–40%, adrenaline by 50–60%, noradrenaline by 45% |
| 19 | V.E. Tseylikman et al., 2018 | Observational | – | In 30% with chronic PTSD ↓ cortisol by 25–30% with ↑ glucocorticoid sensitivity |
| 20 | I.B. Ushakov et al., 2023 | Review | – | Disrupted cortisol diurnal rhythm, ↓ HRV by 20–25%, sleep disturbances |
| 21 | V.M. Lytkin et al., 2024 | Review | – | “Delayed stress”: PTSD manifests after 3–6 months in 62% |
| 22 | S.V. Chepur, 2024 | Review | – | Combat stress → altered microbiota phenotype, ↑ virulence, TLR4 activation |
| 23 | E. Baguma et al., 2024 | Cross‑sectional | 150 (Uganda) | Combat readiness negatively associated with PTSD and alcoholism; alcohol – partial mediator |
| Cluster 2. Contemporary factors | ||||
| 24 | A.G. Karayani, 2024 | Review | – | Definition and classification of combat stress |
| 25 | Z. Bridges‑Curry et al., 2025 | Longitudinal | 783 veterans | Social support buffers stress, but effect disappears at high stress levels |
| 26 | Yu.M. Karayani et al., 2025 | Comparative | 93 SMO participants | Distress linked to antisocial behaviour |
| 27 | M. Grzesik‑Pietrasiewicz et al., 2025 | Experimental | special forces | Stress‑induced neurotransmitter changes |
| 28 | V.I. Evdokimov et al., 2023a | Bibliometric | 894 Russian articles | Analysis of combat stress research directions in Russia |
| 29 | V.I. Evdokimov et al., 2023b | Bibliometric | 5,428 foreign articles | Analysis of international combat stress publications (VOSviewer) |
| Cluster 3. Diagnostics | ||||
| 30 | K.Yu. Telesheva et al., 2024 | Cross‑sectional | 40 (18 PTSD + 22 controls) | ↑ latency of N100, P200, MMN; accuracy 87% |
| 31 | M.S. Pluzhnik et al., 2024 | Comparative | 163 combatants | Mississippi–PC‑PTSD‑5 correlation
(r = 0.588) |
| 32 | T.D. Vasilenko et al., 2025 | Psychosemantic | 46 wounded | In PTSD, situation perceived as unclear but resolvable |
| 33 | A. Efremov, 2025 | Cross‑sectional | 100 US veterans | Age 18–30 – max vulnerability (4.2), 50+ – ↓ vulnerability, ↑ chronification |
| 34 | T.A. Vasilyeva et al., 2023 | Review | – | Diagnostic algorithm for PTSD |
| 35 | N.V. Zelenina et al., 2024 | Comparative | – | Diagnosis of mental disorder level in combatants |
| Cluster 4. Rehabilitation | ||||
| 36 | S.V. Larskikh et al., 2023 | Interventional | 74 combatants | CBT: Mississippi 102→88, anxiety 30→24 |
| 37 | M.G. Volovik et al., 2023 | Syst. review | 75 articles | VRET effective in resistant PTSD (up to 65%) |
| 38 | E.A. Dudina & A.A. Blaginin, 2024 | Experimental | 17 combatants | HHT: ↓ state anxiety (39.7→25.7) |
| 39 | A.B. Adler & I.A. Gutierrez, 2022a | Pre‑post | 129 soldiers | iCOVER: ↑ knowledge (43.5→79.6%), ↑ confidence (64→90%) |
| 40 | Y.Q. Liu et al., 2024 | RCT | 121 sailors | Positive “4C” intervention: PSQI 6.96→4.32; DRS‑II +2.24; GSES +0.5 |
| 41 | J.T. Goodson & G.J. Haeffel, 2022 | Pre‑post (pilot) | 5 veterans | BTAP: ↓ PCL‑5 by 31 points (d = 1.7) |
| 42 | R.H. Schneider et al., 2025 | Commentary | – | Transcendental Meditation: ↓ BP 5–10 mmHg, ↓ cardiovascular events by 48% |
| 43 | R.V. Kadyrov & A.L. Venger, 2021 | Review | – | EMDR effective in complex PTSD (70% remission) |
| 44 | L.N. Kasimova et al., 2024 | Experimental | – | VRET: effectiveness up to 65% |
| 45 | N.V. Dvoryanchikov et al., 2025 | Experimental | – | Folk game practice in correcting avoidance and emotional numbing |
| 46 | Yu.V. Polina et al., 2025 | Review | – | Psychotherapy methods in SMO participants’ rehabilitation |
| 47 | E.V. Pashnin et al., 2025 | Comparative | – | Immune parameters in veterans |
| 48 | I.P. Zaitseva & L.P. Sizyakina, 2016 | Comparative | – | Haematological changes in veterans |
| 49 | A.A. Zuikova et al., 2018 | Comparative | – | Somatoform and reproductive disorders in combatants |
| Cluster 5. Organisational models | ||||
| 50 | A.G. Solovyev et al., 2019 | Review | – | Five‑stage rehabilitation model |
| 51 | A.A. Zhilyaev & D.V. Tipsin, 2018 | Normative review | – | Three‑period rehabilitation in Russian National Guard |
| 52 | N.I. Shempeleva et al., 2026 | Cross‑sectional | 44 pairs | Wife’s readiness for change correlates with veteran adaptation (r = 0.67) |
| 53 | A.G. Karayani et al., 2024 | Review | – | Proactive care model |
| 54 | A.B. Adler & I.A. Gutierrez, 2022b | Review | – | iCOVER, early screening, integration of psychologists |
| 55 | A.G. Karayani & P.S. Protsenko, 2026 | Review | – | Chronification of the “combat self” in veterans |
| 56 | A.G. Karayani et al., 2025 | Review | – | Social expectations as a mechanism for resocialisation |
| 57 | L.N. Fettsova et al., 2024 | Review | – | Methodological approaches to combatant rehabilitation |
| 58 | S.V. Vyaltsin et al., 2025 | Review | – | Frequency of stress‑associated disorders (up to 70%) |
| 59 | H. Shahmiri Barzoki et al., 2021 | Meta‑analysis | – | PTSD prevalence in combatants – 27.8% |
3.2. Neurobiological, genetic and psychological mechanisms of the transition from eustress to distress (Cluster 1)
The first and largest cluster brings together studies elucidating the neurobiological, genetic and psychological mechanisms underlying the transformation of adaptive combat stress (eustress) into pathogenic distress. The key finding from this cluster is the dual nature of combat stress: on one hand, it mobilises the organism, increasing catecholamine and cortisol levels; on the other, when chronic, it leads to exhaustion of the hypothalamic–pituitary–adrenal axis and the development of neuroinflammation (Ushakov et al., 2023; Maslyakov et al., 2025).
Feigel et al. (2025) introduce the concept of allostatic load, showing that the ALI increases by 2–3 points over 10 weeks of intensive training and correlates with decreased physical performance (r = –0.60, p < 0.01). The neuroinflammatory component is confirmed by Tuchina et al. (2018), who documented elevated IL‑1β, IL‑6 and TNF‑α, and by Chepur (2024), who additionally points to altered symbiotic microbiota phenotype and TLR4 activation.
Genetic studies (Nievergelt et al., 2019; Reznik, 2022) have revealed overlapping risk loci for PTSD with schizophrenia and major depression, with FKBP5 polymorphisms associated with increased risk (OR = 1.8). However, a large‑scale cohort study by Wolf et al. (2024) on 138,592 veterans refutes the previously hypothesised moderating role of the APOE ε4 allele, prompting a reassessment of the assumed genetic link between PTSD and Alzheimer’s disease.
Notably, Price et al. (2024) demonstrated that even subclinical PTSD (mean PCL‑M score 25.1) fully mediates the relationship between combat exposure and everyday cognitive errors (β = 0.149), which has critical implications for preventing mistakes in combat settings. Dissociation and somatisation emerged as powerful predictors of severe PTSD: in Shabat et al. (2024), dissociation showed OR = 6.42 and somatisation OR = 4.79.
Moral injury, particularly betrayal events from command, was associated with somatisation (β = 0.26) and anger (β = 0.25) (Campbell et al., 2026). The theoretical “Ajax effect” model (Sagalakova et al., 2025) explains the transition from moral injury to suicidal behaviour through dissociative mechanisms. Professional burnout, as shown by Vetrova et al. (2024), increases with service length (r = 0.57), with tension, exhaustion and emotional burnout significantly higher in those with more than 5 years of service.
Sex differences (Dell et al., 2025) manifest in resilience being the key protective factor for women (aOR = 0.94–0.91), whereas for men it is partnership (aOR = 0.69). Appetitive aggression, found in 58% of retiring Ugandan soldiers (Bigirwa et al., 2025), and alcohol as a partial mediator between combat readiness and PTSD (Baguma et al., 2024) expand our understanding of behavioural risks.
Overall, Cluster 1 convincingly demonstrates that the transition from eustress to distress is a multifactorial process involving neuroendocrine, immune, genetic and psychological components, with subclinical symptoms, dissociative and somatic manifestations, and sex‑ and tenure‑related factors playing critical roles.
3.3. Contemporary factors accelerating the transition from eustress to distress (Cluster 2)
Studies in the second cluster focus on the specific conditions of modern armed conflicts that greatly amplify stress in military personnel. Karayani (2024) identifies key factors distinguishing contemporary combat from past wars. A longitudinal study by Bridges‑Curry et al. (2025) on 783 veterans showed that social support buffers stress, but this protective effect disappears entirely at high stress levels, directly relevant to SMO settings where social isolation and constant life threat neutralise usual support mechanisms. Karayani et al. (2025) found a direct link between distress and antisocial behaviour, including aggression and offending, especially important in the context of prolonged deployment. Experimental studies by Grzesik‑Pietrasiewicz et al. (2025) on special forces revealed significant neurotransmitter changes under stress, pointing to neurochemical bases of behavioural breakdowns. Bibliometric works by Evdokimov et al. (2023a, 2023b) analyse publication trends, showing a shift from medical aspects to socio‑psychological consequences of combat stress.
Six groups of contemporary factors that accelerate the transition from eustress to distress can be identified:
Technological – constant UAV threat, “expectation‑of‑strike syndrome”, sleep disturbances in 78% of personnel;
Informational – fake news, shocking content, “informational PTSD”;
Organisational – 6–12‑month rotations, insufficient rest (3–4 weeks), “rotation syndrome” in 45% of veterans;
Communication paradoxes – video calls with family intensify guilt;
Social – support disappears under high stress;
Genetic vulnerability – FKBP5, DRD2, SLC6A4 polymorphisms.
Thus, Cluster 2 justifies the need to account for technogenic, informational, and organisational features of SMO when designing preventive measures.
3.4. Objective diagnostic methods (Cluster 3)
The third cluster addresses instrumental and laboratory approaches to early detection of PTSD and related conditions. Telesheva et al. (2024) showed that neurophysiological markers (evoked potentials N100, P200 and mismatch negativity,MMN) achieve classification accuracy of up to 87%, opening prospects for objective diagnosis in complex cases. Pluzhnik et al. (2024) established a correlation between the Mississippi Scale and the PC‑PTSD‑5 screening tool (r = 0.588), enabling rapid assessment. Vasilenko et al. (2025), using a psychosemantic approach, found that in PTSD the traumatic situation is perceived as unclear but resolvable, serving as a cognitive marker. Efremov (2025) on 100 US veterans showed age‑related dynamics: maximum vulnerability (4.2 points) occurs in the 18–30 age group, while in those over 50 vulnerability decreases but symptom chronification increases. Vasilyeva et al. (2023) proposed a diagnostic algorithm comprising screening, in‑depth assessment and differential diagnosis. Zelenina et al. (2024) developed methods for diagnosing mental disorder levels in combatants with acute stress disorder during inpatient rehabilitation.
These data support a comprehensive diagnostic protocol combining clinical scales (CAPS‑5, PCL‑5), neurophysiology (evoked potentials) and circulating resilience biomarkers (cortisol AUC 0.78, NPY AUC 0.82, IGF‑1 AUC 0.75). Genetic testing for APOE ε4 is not recommended (Wolf et al., 2024).
Thus, Cluster 3 demonstrates a shift from purely clinical diagnosis to a multidimensional approach incorporating neurophysiological, psychosemantic, and age‑related parameters.
3.5. Psychological rehabilitation methods (Cluster 4)
The fourth cluster compiles studies on the effectiveness of various psychotherapeutic and psychoeducational interventions. Traditional methods such as cognitive‑behavioural therapy (CBT), EMDR, virtual reality exposure therapy (VRET), biofeedback (BFB) and hypobaric hypoxic training (HHT) have solid evidence bases (Larskikh et al., 2023; Kadyrov & Venger, 2021; Volovik et al., 2023; Dudina & Blaginin, 2024). A meta‑analysis of four RCTs confirms CBT superiority over control (SMD = –1.24). The iCOVER protocol (Adler & Gutierrez, 2022a) showed high effectiveness in increasing knowledge (43.5% to 79.6%) and reducing stigma, especially valuable for pre‑deployment prevention. The positive “4C” psychological intervention (Liu et al., 2024) improved sleep quality (PSQI 6.96→4.32) and self‑efficacy (GSES +0.5) in sailors under prolonged isolation. Behavioural therapy for anxiety and PTSD (BTAP) in a pilot study (Goodson & Haeffel, 2022) reduced PCL‑5 by 31 points (Cohen’s d = 1.7), but requires large‑scale RCT confirmation. Transcendental Meditation (Schneider et al., 2025) proved effective as secondary prevention of cardiovascular events (risk reduction 48%), relevant for veterans with comorbid conditions. Folk game practice (Dvoryanchikov et al., 2025) and psychotherapy methods (Polina et al., 2025) add to the rehabilitation arsenal. Immunological and haematological studies (Pashnin et al., 2025; Zaitseva & Sizyakina, 2016) indicate that some interventions may affect peripheral inflammatory markers.
Thus, Cluster 4 demonstrates the existence of both well‑established methods (CBT, EMDR, VRET) and promising new approaches (iCOVER, BTAP, Transcendental Meditation) requiring further investigation.
3.6. Organisational models of care and resocialisation (Cluster 5)
The fifth cluster examines systemic solutions at the military and civilian structure levels. Solovyev et al. (2019) proposed a five‑stage rehabilitation model covering from pre‑deployment training to post‑rehabilitation follow‑up. Zhilyaev and Tipsin (2018) described a three‑period system (preparatory, extreme, recovery) in the Russian National Guard, supported by legal framework (Federal Law No. 226, orders No. 875, No. 515). The proactive model developed by Karayani et al. (2024) and Adler et al. (2022b) includes early screening (“Psychological Risk Map”), iCOVER training in the “red zone”, and integration of psychologists into combat units, showing advantages over the traditional reactive model. Gender‑sensitive programmes (Dell et al., 2025) recommend resilience training for women and partnership support plus anger management for men. Family involvement is a crucial element of resocialisation: Shempeleva et al. (2026) found that the wife’s readiness for change correlates with veteran adaptation (r = 0.67). Karayani and Protsenko (2026) described the chronification of the “combat self” and proposed methods to overcome it. Societal expectations also serve as a mechanism for resocialisation (Karayani et al., 2025). Methodological approaches by Fettsova et al. (2024) and data from Naumova (2023) on high frequency of stress‑associated disorders (up to 70%) underline the magnitude of the problem. The meta‑analysis by Shahmiri Barzoki et al. (2021) provides an overall PTSD prevalence estimate among combatants of 27.8%.
In summary, Cluster 5 justifies the transition to a multimodal, proactive and gender‑sensitive system of care with active family inclusion and consideration of social expectations.
Table 2. Comparative effectiveness of psychological rehabilitation methods (GRADE evidence levels)
| Method | Effectiveness | Level of evidence | Main limitations |
| CBT (trauma‑focused) | 40–60% symptom reduction | 1a | Requires trauma verbalisation |
| EMDR | 50–70% remission | 1a | Requires certification |
| VRET | 30–50% (up to 65% in resistant cases) | 1b | Cost, cybersickness |
| BFB | 25–40% anxiety reduction | 2b | Requires 10–15 sessions |
| HHT | ↓ state anxiety by 30–35% | 2b | Contraindications (CVD, pulmonary) |
| iCOVER | ↑ knowledge by 37%, ↑ confidence by 26%, ↓ stigma | 2b | Does not replace psychotherapy |
| Positive “4C” intervention | PSQI 6.96→4.32; DRS‑II +2.24; GSES +0.5 | 1b | Duration 6 months |
| BTAP | ↓ PCL‑5 by 31 points (d=1.7); ↓ protective behaviour (d=2.2) | 2b (pilot) | Small sample, needs RCT |
| Transcendental Meditation | ↓ BP 5–10 mmHg; ↓ cardiovascular events by 48% | 1b | Requires regular practice |
CBT applied to 74 combatants, participants in SMO, reduced the Mississippi PTSD Scale total score (range 35–175) from 102 to 88, representing a clinically significant improvement (Larskikh et al., 2023). EMDR (eye movement desensitisation and reprocessing) achieves remission in 50–70% of patients, especially effective in complex PTSD (Kadyrov & Venger, 2021). Virtual reality exposure therapy (VRET) shows 30–50% effectiveness, reaching up to 65% in resistant PTSD (Volovik et al., 2023; Kasimova et al., 2024). The iCOVER protocol (60‑minute training) increases knowledge about acute stress from 43.5% to 79.6% correct answers and confidence in one’s actions from 64% to 90% (Adler & Gutierrez, 2022a). Behavioural therapy for anxiety and PTSD (BTAP) targets and eliminates protective behaviours (avoidance, hypervigilance, rituals); therapist training takes 1 day (Goodson & Haeffel, 2022). Transcendental Meditation reduces the risk of cardiovascular events (myocardial infarction, stroke, cardiovascular death) by 48% in secondary prevention among patients with existing heart disease (Schneider et al., 2025). The positive “4C” psychological intervention (control, commitment, confidence, challenge) in sailors under prolonged confinement improved sleep quality (Pittsburgh Sleep Quality Index decreased from 6.96 to 4.32), psychological resilience (increase of 2.24 points on the DRS‑II scale), and self‑efficacy (increase of 0.5 points on the GSES scale) (Liu et al., 2024).
Discussion
The aim of this systematic review was to integrate multi‑level data, from molecular biology to healthcare organisation, in order to elucidate the neurobiological, genetic, psychological and organisational mechanisms that determine the transition from combat stress to pathogenic distress in participants of special military operations (SMOs), and to evaluate objective diagnostic methods and effective rehabilitation interventions. The overarching finding, which runs as a unifying thread through all analysed clusters and constitutes the conceptual core of the present work, is that the transition from adaptive eustress to chronic distress is not driven by any single mechanism but represents a multifactorial process in which the subclinical level of post‑traumatic stress disorder (PTSD) plays a critical role, fully mediating the relationship between combat exposure and everyday cognitive errors (Price et al., 2024). This phenomenon, namely cognitive vulnerability emerging even before PTSD diagnostic criteria are met, acts as the molecular trigger that shifts adaptive responses into a pathological trajectory while simultaneously opening a window for early preventive intervention. The conceptual model proposed by Bukhtiyarov and Glukhov (2020) delineates three sequential levels of transition from combat stress to pathology: adaptive reactions, maladaptive states, and clinically defined disorders. This three‑tiered framework aligns with our central finding regarding the critical role of subclinical PTSD, which occupies a borderline position between adaptation and maladaptation. Unlike previous reviews restricted to neuroendocrine markers (Beckner et al., 2021) or to stress classification without quantitative treatment assessment (Karayani, 2024), the present work demonstrates for the first time that subclinical PTSD serves as a central hub linking combat stress to functional impairments, and that effective prevention should target the detection and correction of preclinical cognitive and affective shifts rather than focusing solely on treating full‑blown disorders.
This central finding must be interpreted within the broader context of neurobiological and genetic mechanisms. First, distress cannot be reduced to simple exhaustion of the hypothalamic–pituitary–adrenal axis (Ushakov et al., 2023). Alongside elevated cortisol, adrenaline, and noradrenaline levels (Maslyakov et al., 2025), neuroinflammation, characterised by elevated IL‑1β, IL‑6 and TNF‑α (Tuchina et al., 2018), and gut microbiota dysbiosis, which potentiates systemic inflammation through Toll‑like receptor activation (Chepur, 2024), make substantial contributions. The concept of allostatic load (Feigel et al., 2025) provides a quantitative measure of cumulative stress burden: a 2–3‑point increase in the ALI over 10 weeks of intensive training correlates with decreased physical performance (r = –0.60). A systematic review by Van Cutsem et al. (2026) synthesised evidence on circulating resilience biomarkers, showing that cortisol (AUC 0.78), neuropeptide Y (AUC 0.82), and insulin‑like growth factor 1 (AUC 0.75) possess good predictive capacity for maintaining psychological resilience under combat stress conditions. These markers may be employed for early identification of service members at elevated risk of adaptation failure. Genetic studies confirm overlapping risk loci for PTSD with schizophrenia and major depression, and FKBP5 polymorphisms are associated with elevated risk (OR = 1.8) (Nievergelt et al., 2019; Reznik, 2022). However, the large‑scale cohort study by Wolf et al. (2024) on 138,592 veterans refutes the moderating role of the APOE ε4 allele, thereby obviating routine testing for this marker and revising the presumed link between PTSD and Alzheimer’s disease. Shelef et al. (2025), in a sample of 927 Israeli veterans, demonstrated that depression (Exp(B) = 3.115) and dissociation (Exp(B) = 1.237) are independent predictors of PTSD, confirming the need for combined screening of depressive and dissociative symptoms. Experimental studies by Grzesik‑Pietrasiewicz et al. (2025) on special forces personnel revealed significant stress‑induced neurotransmitter changes, pointing to neurochemical underpinnings of behavioural dysregulation. Yet, as important as these neuroendocrine, genetic, and neurochemical factors are, it is the subclinical level of PTSD that, according to Price et al. (2024), constitutes the operative link directly connecting combat experience to everyday cognitive errors (β = 0.149). Even mild, sub‑diagnostic symptoms can impair attention and memory, increasing the risk of operational errors. This justifies mandatory screening with the Cognitive Failures Questionnaire (CFQ) for all military personnel, regardless of clinical diagnosis. A clinically important phenomenon requiring consideration in service organisation is “delayed stress”. Lytkin et al. (2024) demonstrated that in 62% of veterans, PTSD manifests 3–6 months after return from the combat zone, dictating the need for extended (at least 12 months) post‑deployment follow‑up. Tseylikman et al. (2018) showed that in 30% of patients with chronic PTSD, cortisol levels decrease by 25–30% with concurrent increase in glucocorticoid sensitivity, indicating hypothalamic–pituitary–adrenal axis exhaustion in later stages of the disorder, in contrast to the acute phase characterised by hypercortisolaemia.
Extending this central result, it becomes necessary to account for psychopathological phenomena that are independent of PTSD severity. Moral injury, encompassing guilt, shame, and betrayal, as well as dissociative and somatic symptoms, independently contribute to suicidal behaviour beyond PTSD severity (Sagalakova et al., 2025; Campbell et al., 2026). Dissociation (OR = 6.42) and somatisation (OR = 4.79) emerged as the strongest predictors of severe PTSD (Shabat et al., 2024). The proposed ‘Ajax effect’ model (Sagalakova et al., 2025) explains how moral injury, through negative affects such as shame, guilt, and entrapment, generates suicidal ideation, whereas dissociation, by reducing pain sensitivity and emotional engagement, catalyses the transition to suicidal action. This necessitates the inclusion of dissociation (DES) and moral injury (MIOS) scales in screening protocols. Thus, the central role of subclinical PTSD is modulated by these moderators, which can accelerate or slow the transition to clinically overt outcomes.
Sex and age differences also modulate this process. Protective factors operate differentially: resilience is key for women (aOR = 0.94–0.91), whereas for men partnership and anger control are more important (aOR = 0.69) (Dell et al., 2025). At high stress levels, the buffering effect of social support completely disappears (Bridges‑Curry et al., 2025). Age dynamics are also critical: maximal vulnerability occurs at 18–30 years (4.2 points), while after 50, despite reduced symptom intensity, chronification and treatment resistance increase (Efremov, 2025). Complementing this age‑related dynamics, Barysheva (2020), in a sample of 150 service members, showed that experienced soldiers, despite reduced overall activity, exhibit higher stress resistance, which may reflect a “training” effect of adaptive mechanisms; however, this is accompanied by increasing professional burnout (Vetrova et al., 2024). Appetitive (hedonistic) aggression, found in 58% of retiring Ugandan soldiers, is associated with harm infliction (aOR = 3.26) and paradoxically unrelated to depression, which may reflect its adaptive role in combat, namely protection against PTSD at the cost of increased violence and antisocial behaviour (Bigirwa et al., 2025). Alcohol partially mediates the link between combat readiness and PTSD (Baguma et al., 2024), mandating alcohol screening in training and rehabilitation programmes. Karayani et al. (2025) demonstrated a direct link between distress and antisocial behaviour, including aggression and offending, which is particularly relevant in the context of prolonged deployment. All these factors, including sex, age, appetitive aggression, alcohol, and antisocial tendencies, interact closely with subclinical PTSD, either amplifying its cognitive and affective consequences or, conversely, masking them through behavioural compensations.
Turning to therapeutic implications, traditional methods, such as cognitive‑behavioural therapy (CBT), EMDR, virtual reality exposure therapy (VRET), biofeedback (BFB), and hypobaric hypoxic training (HHT), have solid evidence bases; a meta‑analysis of four RCTs confirms CBT superiority over control (SMD = –1.24) (Larskikh et al., 2023; Kadyrov & Venger, 2021; Volovik et al., 2023; Dudina & Blaginin, 2024). Kasimova et al. (2024), in an experimental study, confirmed VRET effectiveness in treatment‑resistant PTSD (up to 65% improvement). However, in light of the central role of subclinical PTSD, the most promising interventions are those targeting the preclinical stage. The iCOVER protocol, which consists of a one‑hour training session, increased knowledge about acute stress from 43.5% to 79.6% and significantly reduced stigma, making it suitable for deployment in combat units (Adler & Gutierrez, 2022a). The positive ‘4C’ psychological intervention improved sleep quality (PSQI 6.96→4.32), psychological resilience (DRS‑II +2.24), and self‑efficacy (GSES +0.5) in sailors under prolonged isolation (Liu et al., 2024). Emerging approaches, including behavioural therapy for anxiety and PTSD (BTAP) and Transcendental Meditation, have shown encouraging but preliminary results. BTAP, focusing on eliminating protective behaviours, reduced PCL‑5 by 31 points (Cohen’s d = 1.7), whereas Transcendental Meditation reduced cardiovascular event risk by 48% in secondary prevention (Goodson & Haeffel, 2022; Schneider et al., 2025). Folk game practice, according to Dvoryanchikov et al. (2025), demonstrates effectiveness in correcting avoidance symptoms and emotional numbing in combatants. Psychotherapy methods for SMO participant rehabilitation are summarised by Polina et al. (2025). Furthermore, immunological and haematological studies (Pashnin et al., 2025; Zaitseva & Sizyakina, 2016) indicate that some interventions may influence peripheral inflammatory markers, opening possibilities for monitoring treatment effectiveness at the biochemical level. Nevertheless, BTAP, Transcendental Meditation and folk game practice require large‑scale RCTs with active control groups and long‑term follow‑up. Importantly, all these methods, regardless of their specific nature, should be integrated into a unified system oriented toward early detection of subclinical impairments and their correction before they evolve into clinical pathology.
A comprehensive diagnostic approach requires integration of multiple assessment levels. The psychosemantic study by Vasilenko et al. (2025) showed that in PTSD, the traumatic situation is perceived as unclear but resolvable, which may serve as a cognitive marker. The diagnostic algorithm proposed by Vasilyeva et al. (2023) comprises screening, in‑depth assessment and differential diagnosis, while Zelenina et al. (2024) developed methods for diagnosing the level of mental disorders during inpatient rehabilitation. For field screening, Pluzhnik et al. (2024) established a correlation between the Mississippi Scale and the PC‑PTSD‑5 questionnaire (r = 0.588), allowing the latter to be used for rapid assessment. The most promising objective methods are neurophysiological markers: Telesheva et al. (2024) demonstrated that evoked potentials N100, P200 and mismatch negativity (MMN) achieve PTSD classification accuracy of up to 87%. Collectively, these data support a multi‑level diagnostic protocol combining clinical scales, neurophysiological methods and circulating biomarkers.
From an organisational perspective, comparison of approaches reveals the clear superiority of a proactive multimodal model, including early biomarker screening, iCOVER training in the ‘red zone’, integration of psychologists into combat units and gender‑sensitive programmes, over the traditional reactive model focused on treating already developed disorders after return (Karayani et al., 2024; Adler & Gutierrez, 2022b). In Russian practice, two main organisational models have been tested: the three‑period system (preparatory, extreme, recovery periods) proposed by Zhilyaev and Tipsin (2018) for the Russian National Guard, and the five‑stage rehabilitation model by Solovyev et al. (2019), covering the period from pre‑deployment training to post‑rehabilitation support. Vyaltsin et al. (2025), in a literature review, showed that the frequency of stress‑associated disorders in combatants reaches 70%, confirming the scale of the problem and the need for systemic organisational solutions. Karayani and Protsenko (2026) described the phenomenon of chronification of the “combat self” in veterans, whereby identity formed under conditions of constant threat persists after return to civilian life, impeding full resocialisation. Overcoming this phenomenon requires specialised psychotherapeutic interventions aimed at integrating combat experience into a new life perspective. Family involvement, where the wife’s readiness for change correlates with veteran adaptation (r = 0.67), and the creation of positive social expectations, such as the perception of the ‘veteran‑hero’, are crucial components of resocialisation (Shempeleva et al., 2026; Karayani et al., 2025). Methodological approaches by Fettsova et al. (2024) synthesise contemporary strategies for medical‑psychological correction and rehabilitation of combatants. A meta‑analysis by Shahmiri Barzoki et al. (2021) provides an overall PTSD prevalence estimate among combatants of 27.8%, highlighting the systemic nature of the problem. Evdokimov et al. (2023a, 2023b), in bibliometric studies, analysed scientific publication trends, showing a shift from medical aspects to socio‑psychological consequences of combat stress, confirming the relevance of our integrative approach. It is the proactive model, being aimed at preclinical stages, that best aligns with the central finding of this review, namely the key role of subclinical PTSD and cognitive impairments as early targets for prevention.
In summary, the synthesis of the obtained data allows us to formulate six main conclusions. First, combat stress has a dual nature, and the transition to distress is driven by exhaustion of neuroendocrine mechanisms, neuroinflammation, dysbiosis, genetic predisposition, including FKBP5 polymorphisms, and GWAS overlap with schizophrenia and depression, as well as epigenetic changes; however, APOE ε4 is not a moderator of the association between combat stress and PTSD (Wolf et al., 2024; Chepur, 2024; Nievergelt et al., 2019; Reznik, 2022). Second, subclinical PTSD fully mediates the relationship between combat exposure and cognitive errors, justifying mandatory CFQ screening (Price et al., 2024) and serving as the central hub around which the entire system of early diagnosis and prevention should be built. Third, sex differences are critical: resilience is the key protective factor for women, whereas for men partnership and anger control are more important; moreover, social support buffers stress only up to a certain level (Dell et al., 2025; Bridges‑Curry et al., 2025). Fourth, appetitive aggression was found in 58% of retiring soldiers and is associated with harm infliction (aOR = 3.26); alcohol, in turn, partially mediates the link between combat readiness and PTSD (Bigirwa et al., 2025; Baguma et al., 2024). Fifth, effective rehabilitation methods include CBT (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65% in resistant forms), BFB, HHT, iCOVER (knowledge increase by 37%), positive interventions, BTAP (PCL‑5 reduction by 31 points, d = 1.7), Transcendental Meditation (cardiovascular risk reduction by 48%) and folk game practice. Sixth, the proactive multimodal care model, integrating early screening, ‘red zone’ training and family involvement, is significantly more effective than the reactive one (Adler & Gutierrez, 2022b; Karayani et al., 2024), and it should become the organisational foundation for implementing early screening and prevention of subclinical impairments.
Future research directions emerge directly from the identified gaps. Large‑scale multicentre RCTs are needed to evaluate the effectiveness of BTAP, Transcendental Meditation, folk game practice, and the burnout correction programme (Vetrova et al., 2024) with active control groups and long‑term follow‑up (at least 12 months). Longitudinal genetic‑epigenetic studies with repeated biomarker measurements, including cortisol, NPY, IL‑6, and TNF‑α, before, during and after combat deployment, are required to establish causal relationships. Investigation of appetitive aggression and antisocial behaviour in Russian combatant samples using validated instruments, such as the AAS and Patrick’s test, along with analysis of culturally specific factors, is necessary. In‑depth exploration of sex difference mechanisms, encompassing hormonal, neurobiological, and psychosocial aspects, will enable the development of gender‑specific prevention programmes. Validation and adaptation of Russian versions of screening tools, including DES, MIOS, AAS and CFQ, on representative military samples is critically important. The use of wearable devices, such as fitness trackers and pulse oximeters, for continuous monitoring of heart rate variability, sleep quality, and physical activity, with the aim of early detection of allostatic load, is promising. Ecological momentary assessment (EMA) would allow the study of stress dynamics and coping strategies in real combat conditions. Development and testing of proactive multimodal psychological support programmes integrated into combat training and post‑deployment rehabilitation systems, with effectiveness evaluation in quasi‑experimental designs, is needed. Inclusion of combatants’ families in future research is important to assess the role of spousal and social support as a buffer against post‑traumatic stress (Shempeleva et al., 2026). Finally, long‑term consequences of combat stress, covering a period of 5–10 years and including the risk of cardiovascular disease, autoimmune disorders, and accelerated ageing, should be investigated using allostatic load methods (Feigel et al., 2025). Implementation of these directions will enable a transition to personalised prevention and treatment of PTSD in combatants, based on early detection of subclinical cognitive and affective impairments, which constitutes the central finding of this review.
This review has several limitations, including heterogeneity of samples, the small number of RCTs (7 out of 59), predominance of male samples, insufficient genetic data beyond European and African‑American populations, the pilot nature of BTAP, Transcendental Meditation, and folk game practice studies, and the lack of long‑term data for new interventions. Nevertheless, the systematic nature of the review, strict selection criteria, and use of quality assessment tools, in particular JBI, allow the conclusions to be considered reliable and representative for formulating practical recommendations and identifying directions for future research.
Conclusions
This systematic review, synthesising 59 studies with a total participant pool exceeding 18,000 individuals, provides the first comprehensive conceptual framework for understanding the transition from combat stress to pathogenic distress in participants of special military operations. The integration of multi‑level data, from molecular biology to healthcare organization, has identified the central hub of this process: the subclinical level of post‑traumatic stress disorder (PTSD), which fully mediates the relationship between combat exposure and everyday cognitive errors (Price et al., 2024). This phenomenon, previously unexamined in a systematic manner, represents a critical threshold beyond which adaptive responses give way to clinically significant pathology, while simultaneously opening a window for early preventive intervention.
The synthesis of the data obtained demonstrates that the transition from eustress to distress is a multifactorial process involving neuroendocrine mechanisms (hypothalamic–pituitary–adrenal axis exhaustion, elevated cortisol and catecholamine levels), immune dysregulation (neuroinflammation with elevated IL‑1β, IL‑6 and TNF‑α, gut microbiota dysbiosis), genetic predisposition (FKBP5 polymorphisms, overlapping risk loci with schizophrenia and depression) and psychological factors (dissociation, somatisation, moral injury). Notably, the APOE ε4 allele does not moderate the association between combat stress and PTSD, obviating the need for routine testing for this marker (Wolf et al., 2024).
Clinically significant findings demonstrate that dissociation (OR = 6.42) and somatisation (OR = 4.79) represent the strongest independent predictors of severe PTSD, while moral injury, through mechanisms of shame, guilt and entrapment, generates suicidal risk, with dissociation catalysing the transition from suicidal ideation to action (the ‘Ajax effect’ model) (Shabat et al., 2024; Sagalakova et al., 2025). Sex and age differences modulate this process: psychological resilience is the key protective factor for women, whereas partnership and anger control are more important for men; maximal vulnerability occurs at 18–30 years, while after age 50 chronification and treatment resistance increase (Dell et al., 2025; Efremov, 2025). Appetitive aggression, identified in 58% of retiring soldiers, and alcohol as a partial mediator between combat readiness and PTSD expand our understanding of behavioural risks requiring screening (Bigirwa et al., 2025; Baguma et al., 2024).
Practical recommendations arising from this review include mandatory screening using the Cognitive Failures Questionnaire (CFQ) for all military personnel regardless of clinical diagnosis, as well as inclusion of dissociation (DES), moral injury (MIOS), and alcohol screening scales in screening protocols. The diagnostic algorithm should be multi‑level, combining clinical scales (CAPS‑5, PCL‑5), neurophysiological methods (evoked potentials N100, P200, MMN, achieving up to 87% accuracy) and circulating resilience biomarkers (cortisol, NPY, IGF‑1). The rehabilitation strategy should rely on methods with proven effectiveness such as cognitive‑behavioural therapy (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65% in resistant forms), and emerging approaches requiring further investigation in large‑scale RCTs (iCOVER, BTAP, Transcendental Meditation, folk game practice). Organisationally, priority should be given to a proactive multimodal model incorporating early biomarker screening, ‘red zone’ training, integration of psychologists into combat units, gender‑sensitive programmes and active family involvement. It is this model, targeting preclinical stages, that best aligns with the central finding of this review is the critical role of subclinical PTSD and cognitive impairments as early targets for prevention.
Future research should focus on large‑scale multicentre RCTs of novel methods, longitudinal genetic‑epigenetic studies with repeated biomarker measurements before, during, and after combat deployment, investigation of appetitive aggression and antisocial behaviour in Russian samples, validation and adaptation of screening tools, use of wearable devices for continuous allostatic load monitoring, and ecological momentary assessment to study stress dynamics in real combat conditions. Implementation of these directions will enable a transition to personalised prevention and treatment of PTSD in combatants, based on early detection of subclinical impairments.
Competing interests: The authors declare no competing interests in relation to the publication of this manuscript.
Funding: The study was carried out within the framework of the state assignment “Intelligent Systems and Human Abilities” – No. 0138-2026-0016. Registration number in the Unified State Information System for Accounting Research, Development and Technological Work (EGISU NIOTKR): 1023033000550-6-5.1.1.
Acknowledgements: The authors thank reviewers for valuable comments and consultative support during manuscript preparation.
Author Contributions: A. M. Babaev and N. E. Volkova contributed equally to the conceptualisation, data collection and analysis, writing and editing of the manuscript.
AI Usage Statement: Artificial intelligence was used for final text editing of the manuscript to enhance its clarity and literary quality. All scientific statements, data and conclusions are the result of the authors’ independent work.
References
- Adler, A. B., & Gutierrez, I. A. (2022a). Preparing soldiers to manage acute stress in combat: Acceptability, knowledge and attitudes. Psychiatry, 85(1), 30–37. https://doi.org/10.1080/00332747.2021.2021598
- Adler, A. B., & Gutierrez, I. A. (2022b). Acute stress reaction in combat: Emerging evidence and peer‑based interventions. Current Psychiatry Reports, 24(4), 277–284. https://doi.org/10.1007/s11920-022-01335-2
- Baguma, E. A., Vivalya, B. M. N., Ocen, P. O., & Kasujja, R. (2024). Combat readiness, alcohol abuse, and posttraumatic stress disorder among Uganda peoples’ defence forces soldiers. BMC Psychology, 12(1), Article 581. https://doi.org/10.1186/s40359-024-02068-y
- Barysheva, E. I. (2020). Stress resistance of military personnel in local armed conflict conditions. Penza Psychological Bulletin, 1(14), 50–63. https://doi.org/10.17689/psy-2020.1.5[in Russian]
- Beckner, M. E., Conkright, W. R., Eagle, S. R., Martin, B. J., Sinnott, A. M., La Goy, A. D., & Nindl, B. C. (2021). Impact of simulated military operational stress on executive function relative to trait resilience, aerobic fitness, and neuroendocrine biomarkers. Physiology & Behavior, 236, Article 113413. https://doi.org/10.1016/j.physbeh.2021.113413
- Bigirwa, D. M., Rukundo, G. Z., Muwanguzi, M., Favina, A., & Ashaba, S. (2025). Appetitive aggression and associated factors among military soldiers retiring from active service in Uganda. European Journal of Psychotraumatology, 16(1), Article 2493026. https://doi.org/10.1080/20008066.2025.2493026
- Bridges‑Curry, Z., Meckes, S. J., Fountain, C., Wagner, H. R., Calhoun, P. S., Kimbrel, N. A., Rowland, J. A., Dedert, E. A., Ponzini, G. T., & VA Mid‑Atlantic MIRECC Workgroup. (2025). Combat exposure, social support, and posttraumatic stress: A longitudinal test of the stress‑buffering hypothesis among veterans of the wars in Afghanistan and Iraq. Social Psychiatry and Psychiatric Epidemiology, 60(10), 2495–2504. https://doi.org/10.1007/s00127-025-02864-w
- Bukhtiyarov, I. V., & Glukhov, D. V. (2018). Posttraumatic stress disorder formation in military officers in combat circumstances. Russian Journal of Occupational Health and Industrial Ecology, 2, 10–14. https://doi.org/10.31089/1026-9428-2018-2-10-14[in Russian]
- Campbell, G. M., Biscoe, N., Bonson, A., & Murphy, D. (2026). Association of potential morally injurious events, moral injury and somatic symptoms of health in UK military veterans: A cross‑sectional study. BMC Psychology, 14, Article 56. https://doi.org/10.1186/s40359-025-03788-5
- Chepur, S. V. (2024). Combat stress: Formation mechanisms and targets of directed pharmacological effects. Human Physiology, 50(6), 657–663. https://doi.org/10.1134/S0362119724701123
- Dell, L., Madden, K., Baur, J., Sbisa, A., McFarlane, A., VanHooff, M., Bryant, R., & Lawrence‑Wood, E. (2025). Trauma, resilience and significant relationships: Sex differences in protective factors for military mental health. Australian & New Zealand Journal of Psychiatry, 59(1), 48–59. https://doi.org/10.1177/00048674241286818
- Dudina, E. A., & Blaginin, A. A. (2024). Dynamics of anxiety of combatants during the course of hypobaric hypoxic training. Psychology in Education, 6(2), 210–222. https://doi.org/10.33910/2686-9527-2024-6-2-210-222[in Russian]
- Dvoryanchikov, N. V., Teplova, A. B., & Chernushevich, V. A. (2025). The rehabilitation potential of folklore games in correcting symptoms of avoidance and emotional numbing in combatants. Psychology and Law, 15(4), 20–43. https://doi.org/10.17759/psylaw.2025150001[in Russian]
- Efremov, A. (2026). Age‑specific mental health profiles of combat veterans: Post‑traumatic stress disorder and related disorders. Journal of Rational‑Emotive & Cognitive‑Behavior Therapy, 44, Article 4. https://doi.org/10.1007/s10942-025-00637-7
- Evdokimov, V. I., Shamrey, V. K., & Pluzhnik, M. S. (2023a). Combat stress research prospects in Russian academic publications analyzed using VOSviewer software (2005–2021). Medico‑Biological and Socio‑Psychological Problems of Safety in Emergency Situations, 2, 99–116. https://doi.org/10.25016/2541-7487-2023-0-2-99-116[in Russian]
- Evdokimov V.I., Shamrey V.K., Pluzhnik M.S. Combat stress research prospects in Russian academic publications analyzed using to VOSviewer software (2005–2021). Medicо-Biological and Socio-Psychological Problems of Safety in Emergency Situations. 2023;(2):99-116. (In Russ.) https://doi.org/10.25016/2541-7487-2023-0-2-99-116
- Feigel, E. D., Koltun, K. J., Lovalekar, M., Friedl, K. E., Martin, B. J., & Nindl, B. C. (2025). Advancing the allostatic load model in military training research: From theory to application. Frontiers in Physiology, 16, Article 1638451. https://doi.org/10.3389/fphys.2025.1638451
- Fettsova, L. N., Serova, Yu. S., & Yusupov, V. V. (2024). Methodological approaches to combatants’ medical and psychological correction and rehabilitation. Living Psychology, 11(5), 10–18. https://doi.org/10.58551/24136522_2024_11_5_10[in Russian]
- Goodson, J. T., & Haeffel, G. J. (2022). Treating posttraumatic stress disorder in combat veterans: A guide to using behavior therapy for anxiety and PTSD (BTAP). Clinical Psychology and Special Education, 11(2), 63–80. https://doi.org/10.17759/cpse.2022110204
- Grzesik‑Pietrasiewicz, M., Łach, K., Brożyna, M., Przednowek, K., & Podgórski, R. (2025). The impact of SERE training on selected neurotransmitter secretion in special forces soldiers. Scientific Reports, 15, Article 21853. https://doi.org/10.1038/s41598-025-06270-9
- Kadyrov, R. V., & Venger, V. V. (2021). Complex post‑traumatic stress disorder: Modern approaches to definition of the concept, etiology, diagnostics, and psychotherapy. Psychologist, 4, 45–60. https://doi.org/10.25136/2409-8701.2021.4.35811[in Russian]
- Karayani, A. G. (2024). Combat stress: Problems of definition and classification. Bulletin of the Moscow University of the Ministry of Internal Affairs of Russia, 1, 254–264. https://doi.org/10.24412/2073-0454-2024-1-254-264[in Russian]
- Karayani, A. G., Protsenko, S. A., & Trofimov, N. V. (2025). Social expectations in society as a mechanism for the re‑socialization of combatants. Psychopedagogy in Law Enforcement, 30(4), 378–391. https://doi.org/10.24412/1999-6241-2025-4103-378-391[in Russian]
- Karayani, A. G., & Protsenko, S. A. (2026). “Never returned from the war”: Phenomenon of chronicization of the combat Ego in veterans of combat operations. Extreme Psychology and Personal Safety, 3(1), 210–224. https://doi.org/10.17759/epps.2026030111[in Russian]
- Karayani, Yu. M., Erokhina, A. V., Milcharek, T. P., & Ivanyuk, V. I. (2025). The relationship between the propensity for antisocial behavior and the type of stress response in servicepersons involved in combat operations. Russian Military Psychology Journal, 2(8), 39–45. https://doi.org/10.25629/RMPJ.2025.02.03[in Russian]
- Kasimova, L. N., Kuznetsov, A. N., Kropinova, I. I., Kuznetsov, D. V., Volovik, M. G., Svyatogor, M. V., Sychugov, E. M., Borovskoy, G. Yu., & Khalak, M. E. (2024). Comprehensive assessment of combatants’ psychological and psychophysiological state in exposure therapy of post‑traumatic stress disorder using virtual reality. Modern Technologies in Medicine, 16(5), 35–44. https://doi.org/10.17691/stm2024.16.5.04[in Russian]
- Kuvaeva, I. O., & Volkova, E. V. (2024). Neurochemical markers of coping intelligence. Kazan Medical Journal, 105(2), 260–271. https://doi.org/10.17816/KMJ623568
- Larskikh, S. V., Larskikh, M. V., Mikhan, O. Yu., Potapova, O. N., & Zheleznyakov, M. A. (2023). A study of the effectiveness of interdisciplinary medical care for combatants with PTSD. Medical Psychology in Russia, 15(4), 21–30. [in Russian]
- Liu, Y. Q., Sun, J. L., Jing, M., Liu, G. X., Shi, J., Zhu, X. W., Wang, F., & Ye, M. H. (2024). Effects of positive psychological control intervention on sleep and psychology of officers and soldiers working at sea. World Journal of Psychiatry, 14(10), 1538–1546. https://doi.org/10.5498/wjp.v14.i10.1538
- Lytkin, V. M., Zun, S. A., Kolodin, S. N., & Yatmanov, A. N. (2024). Post‑combat personality changes in combat veterans. Psychology and Psychotechnics, 4. https://doi.org/10.7256/2454-0722.2024.4.69677[in Russian]
- Maslyakov, V. V., Sidelnikov, S. A., Onishchenko, A. N., Barachevskiy, Yu. E., Zakharova, N. B., Verizhnikova, E. V., Shilova, N. A., Fokht, Yu. V., Burekeshev, A. E., & Romanova, I. V. (2025). Hormonal changes and their relation to psychophysiological parameters in combatants. Disaster Medicine, 3, 83–87. https://doi.org/10.33266/2070-1004-2025-3-83-87[in Russian]
- Nievergelt, C. M., Maihofer, A. X., Klengel, T., et al. (2019). International meta‑analysis of PTSD genome‑wide association studies identifies sex‑ and ancestry‑specific genetic risk loci. Nature Communications, 10, Article 4558. https://doi.org/10.1038/s41467-019-12576-w
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo‑Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Pashnin, S. L., Davydova, E. V., & Altman, D. Sh. (2024). Neurocytokine blood profile of veterans of modern combat conflicts with post‑traumatic stress disorder. Russian Journal of Immunology, 27(2), 343–350. https://doi.org/10.46235/1028-7221-16669-NBP[in Russian]
- Pluzhnik, M. S., Evdokimov, V. I., & Shamrey, V. K. (2024). Assessment of mental adaptation disorders for psychological correction tasks in combatants of the special military operation. Bulletin of Psychotherapy, 91, 95–101. https://doi.org/10.25016/2782-652X-2024-0-91-95-101[in Russian]
- Polina, Yu. V., Kuzmina, A. E., & Surikova, A. A. (2026). Psychotherapy methods in the rehabilitation of participants in a special military operation. Universum: Medicine and Pharmacology, 4(133). https://7universum.com/ru/med/archive/item/22396[in Russian]
- Price, M. M., Zanesco, A. P., Denkova, E., & Jha, A. P. (2024). Examining factors associated with self‑reported cognitive functioning in elite military settings: Considerations of combat experiences and post‑traumatic stress symptomology. Scientific Reports, 14, Article 19161. https://doi.org/10.1038/s41598-024-65826-3
- Reznik, A. M. (2022). Overview of research on external factors and genetic predispositions of combat‑related post‑traumatic stress disorder. Bulletin of the Medical Institute of Continuing Education, 4, 46–55. https://doi.org/10.46393/27821714[in Russian]
- Sagalakova, O. A., Truevtsev, D. V., & Zhirnova, O. V. (2025). “The Ajax effect”: The role of moral injury‑related dissociation in the formation of suicidal behavior during combat stress. Psychology and Law, 15(4), 275–297. https://doi.org/10.17759/psylaw.2025150415[in Russian]
- Schneider, R. H., Norris, K. C., & Brook, R. D. (2026). Transcendental meditation to combat psychosocial stress, hypertension and cardiovascular disease. Nature Reviews Cardiology, 23(1), 4–5. https://doi.org/10.1038/s41569-025-01235-x
- Shabat, N., Bechor, U., Yavnai, N., Tatsa‑Laur, L., & Shelef, L. (2024). The link between somatization and dissociation and PTSD severity in veterans who sought help from the IDF combat stress reaction unit. Military Medicine, 189(11–12), e2562–e2572. https://doi.org/10.1093/milmed/usae118
- Shahmiri Barzoki, H., Ebrahimi, M., Khoshdel, A., et al. (2021). Studying the prevalence of PTSD in veterans, combatants and freed soldiers of Iran‑Iraq War: A systematic and meta‑analysis review. Psychology, Health and Medicine, 28(3), 812–818. https://doi.org/10.1080/13548506.2021.1981408
- Shamrey, V. K., Kurasov, E. S., Kolchev, A. I., & Starostina, E. V. (2025). Combat mental pathology: From evolution of views to modern concepts. Russian Journal of Psychiatry, 1, 5–12. [in Russian]
- Shelef, L., Spira, N., Bechor, U., Rotschield, J., & Shadach, E. (2025). The roles of dissociation and depression in PTSD among soldiers exposed to combat. International Journal of Environmental Research and Public Health, 22(6), 814. https://doi.org/10.3390/ijerph22060814
- Shempeleva, N. I., Pestova, I. V., & Trifonova, N. I. (2026). Psychological resources of the family as a condition for adaptation of veterans (participants) of the special military operation. Bulletin of Practical Psychology of Education, 23(1), 61–75. https://doi.org/10.17759/bppe.2026230104[in Russian]
- Soloviev, A. G., Ichitovkina, E. G., Zlokazova, M. V., Davydova, N. E., & Evdokimov, V. I. (2019). Organization of treatment and rehabilitation for combatants with borderline mental disorders. Ekologiya cheloveka (Human Ecology, 26(5), 60-64. doi: 33396/1728-0869-2019-5-60-64
- Telesheva, K. Yu., Savenkova, V. I., Morozova, I. O., Ochneva, A. G., Zeltser, A. I., Andreyuk, D. S., Reznik, A. M., Mukhin, V. N., Melkonyan, G. G., Lytkina, K. A., Mitrofanov, A. A., & Morozova, A. Yu. (2024). Potential neurophysiological markers of combat‑related post‑traumatic stress disorder. Consortium Psychiatricum, 5(2), CP15512. https://doi.org/10.17816/CP1552[in Russian]
- Tseylikman, V. E., Tseylikman, O. B., Feklicheva, I. V., Maslennikova, E. P., Chipeeva, N. A., & Glukhova, V. A. (2018). Psychological, neurobiological and neuroendocrinological features of post‑traumatic stress disorder syndrome. Bulletin of SUSU. Series “Psychology”, 11(4), 73–86. https://doi.org/10.14529/psy180408[in Russian]
- Tuchina, O. P., Sidorova, M. V., Turkin, A. V., Shvayko, D. A., Shalaginova, I. G., & Vakolyuk, I. A. (2018). Molecular mechanisms of initiation and development of neuroinflammation in a model of post‑traumatic stress disorder. Genes and Cells, 13(2), 47–55. [in Russian]
- Ushakov, I. B., Kalmanov, A. S., & Bubeev, Yu. A. (2023). Prospects for the use of xenon‑based special gas mixtures for stress correction in lethal force situations. Medico‑Biological and Socio‑Psychological Problems of Safety in Emergency Situations, 1, 59–67. https://doi.org/10.25016/2541-7487-2023-0-1-59-67[in Russian]
- Van Cutsem, J., van den Berg, N. H., Flores, B., Aïdara, Y., Martin, A., Musat, A., Pattyn, N., & Simonelli, G. (2026). Circulating biomarkers of military‑specific performance resilience: A systematic review. Current Psychiatry Reports, 28(1), 14. https://doi.org/10.1007/s11920-025-01652-2
- Vasilenko, T. D., Petrachevskaya, Yu. L., Smirnov, N. V., & Gulakov, D. A. (2025). Perception of traumatic events by combatants. RSUH Bulletin: Series Psychology. Education, 2, 151–165. https://doi.org/10.28995/2073-6398-2025-2-151-165[in Russian]
- Vasilyeva, A. V., Karavaeva, T. A., Radionov, D. S., & Starunskaya, D. A. (2023). Diagnostic algorithm for post‑traumatic stress disorder. M. Bekhterev Review of Psychiatry and Medical Psychology, 57(1), 83–95. https://doi.org/10.31363/2313-7053-2023-741[in Russian]
- Vetrova, T. V., Leontyev, O. V., Iontsev, V. I., Yakovlev, E. V., & Trokhmanenko, S. V. (2024). The effect of duration of military service on the psycho‑emotional state of military personnel. Bulletin of Psychotherapy, 91, 102–113. https://doi.org/10.25016/2782-652X-2024-0-91-102-113[in Russian]
- Volovik, M. G., Belova, A. N., Kuznetsov, A. N., et al. (2023). Use of virtual reality techniques to rehabilitate military veterans with post‑traumatic stress disorder (review). Modern Technologies in Medicine, 15(1), 74–86. https://doi.org/10.17691/stm2023.15.1.08[in Russian]
- Vyaltsin, S. V., Mirzayeva, M. V., Semenova, N. V., Vdovichenko, O. V., Pyatkin, A. A., & Dvornikov, I. G. (2025). Acute post‑traumatic stress disorder associated with combat stress (literature review). Specialized Healthcare Services, *85*(2), 31–36. https://doi.org/10.56685/18120555_2025_85_2_31[in Russian]
- Wolf, E. J., Miller, M. W., Zhang, R., et al. (2024). No replication of Alzheimer’s disease genetics as a moderator of the association between combat exposure and PTSD risk in 138,592 combat veterans. Nature Mental Health, 2, 553–561. https://doi.org/10.1038/s44220-024-00225-1
- Zaitseva, N. S., & Sizyakina, L. P. (2023). Characteristics of cytokine imbalance in chronic comorbid stress‑induced disorders in combatants in the long‑term follow‑up period. Immunologiya, 44(3), 326–332. https://doi.org/10.33029/0206-4952-2023-44-3-326-332[in Russian]
- Zelenina, N. V., Chernyavsky, E. A., Fedotkina, I. V., Starenchenko, Yu. L., & Yusupov, V. V. (2024). Diagnostics of the level of mental disorders in combatants with acute stress disorder at the stage of hospital rehabilitation. Clinical and Special Psychology, 13(2), 46–60. https://doi.org/10.17759/cpse.2024130203[in Russian]
- Zhilyaev, A. A., & Tipsin, D. V. (2018). The problem of combat stress and rehabilitation of servicemen of the National Guard of the Russian Federation performing service‑combat tasks. Bulletin of the Russian New University. Series: Man in the Modern World, 1, 29–38. https://doi.org/10.25586/RNU.V925X.18.01.P.029[in Russian]
Comments (0)
Relevance and Background. Participation in special military operations (SMOs) is associated with chronic combat stress, which in a substantial proportion of military personnel transforms into distress and post‑traumatic stress disorder (PTSD). The accumulated body of fragmented data on the mechanisms of this transition requires systematic synthesis to develop effective prevention and rehabilitation strategies. Objective is to integrate data on the neurobiological, genetic, psychological, and organisational mechanisms underlying the transition from combat stress to pathogenic distress in SMO participants, and to evaluate objective diagnostic methods and effective rehabilitation interventions. Methods. This systematic review was conducted in accordance with PRISMA 2020 guidelines. A systematic search was performed across seven databases (PubMed, Web of Science, Scopus, PsycINFO, Google Scholar, eLibrary, RSCI). A total of 59 studies were included (30 Russian, 29 international) with a total participant pool exceeding 18,000. Quality was assessed using the JBI tool. A narrative synthesis was conducted across five clusters, with evidence quality evaluated using the GRADE system. Results. The central hub of the eustress‑to‑distress transition is the subclinical level of PTSD, which fully mediates the relationship between combat exposure and cognitive errors (β = 0.149). Contributing mechanisms include neuroendocrine dysregulation (hypothalamic–pituitary–adrenal axis exhaustion, cortisol elevation by 35–40%), neuroinflammation (IL‑1β, IL‑6, TNF‑α), gut microbiota dysbiosis, and genetic predisposition (FKBP5 polymorphisms, OR = 1.8; GWAS overlap with schizophrenia and depression). APOE ε4 is not a moderator. Dissociation (OR = 6.42) and somatisation (OR = 4.79) are the strongest predictors of severe PTSD. Moral injury, through shame and guilt mechanisms, generates suicidal risk; appetitive aggression was identified in 58% of retiring soldiers. Effective rehabilitation methods include CBT (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65%), iCOVER (knowledge increase by 37%) and BTAP (PCL‑5 reduction by 31 points, d = 1.7). The proactive multimodal care model is significantly more effective than the reactive model. Conclusion. The transition from combat stress to distress is a multifactorial process, with subclinical PTSD serving as its central hub. Early detection of cognitive impairments, dissociation and moral injury enables prevention of disorder chronification. Priority should be given to a proactive multimodal model of psychological care integrated into combat training and post‑deployment rehabilitation systems.
Нейровоспалительные и психосоциальные детерминанты перехода от боевого стресса к дистрессу в условиях современных военных конфликтов: систематический обзор литературы (2018–2026)
А. М. Бабаевa & Н. Е. Волковаb
a Институт синергии, Москва, Россия
bИнститут психологии Российской академии наук, Москва, Россия
Актуальность. Участие в военной операции сопряжено с хроническим боевым стрессом, который у значительной части военнослужащих трансформируется в дистресс и посттравматическое стрессовое расстройство (ПТСР). Накопленный массив разрозненных данных о механизмах этого перехода требует систематизации для разработки эффективных стратегий профилактики и реабилитации. Цель: Интеграция данных о нейробиологических, генетических, психологических и организационных механизмах перехода боевого стресса в патогенный дистресс у участников СВО, а также оценка объективных методов диагностики и эффективных реабилитационных вмешательств. Методы. Систематический обзор выполнен в соответствии с PRISMA 2020. Поиск проведён в семи базах данных (PubMed, Web of Science, Scopus, PsycINFO, Google Scholar, eLibrary, РИНЦ). Включены 59 исследований (30 российских, 29 зарубежных) с общей численностью участников более 18 000 человек. Качество оценено с использованием инструмента JBI. Проведён нарративный синтез по пяти кластерам с применением GRADE для оценки доказательности. Результаты. Центральным звеном перехода эустресса в дистресс является субклинический уровень ПТСР, полностью опосредующий связь боевого опыта с когнитивными ошибками (β = 0,149). В процессе участвуют нейроэндокринные механизмы (истощение гипоталамо-гипофизарно-надпочечниковой оси, повышение кортизола на 35–40%), нейровоспаление (IL‑1β, IL‑6, TNF‑α), дисбиоз микробиоты, генетическая предрасположенность (полиморфизмы FKBP5, OR = 1,8; перекрытие GWAS с шизофренией и депрессией). APOE ε4 не является модератором. Диссоциация (OR = 6,42) и соматизация (OR = 4,79) являются сильнейшими предикторами тяжёлого ПТСР. Моральная травма через механизмы стыда и вины формирует суицидальный риск; аппетитивная агрессия выявлена у 58% уходящих солдат. Эффективные методы реабилитации: КПТ (SMD = –1,24), EMDR (50–70% ремиссии), VRET (до 65%), iCOVER (повышение знаний на 37%), BTAP (снижение PCL‑5 на 31 балл, d = 1,7). Проактивная мультимодальная модель помощи значительно эффективнее реактивной. Заключение. Переход от боевого стресса к дистрессу представляет собой многофакторный процесс, центральным звеном которого выступает субклинический ПТСР. Раннее выявление когнитивных нарушений, диссоциации и моральной травмы позволяет предотвратить хронификацию расстройства. Приоритетной является проактивная мультимодальная модель психологической помощи, интегрированная в систему боевой подготовки и послебоевой реабилитации.
Ключевые слова: боевой стресс, посттравматическое стрессовое расстройство, дистресс, когнитивные ошибки, субклинический ПТСР, диссоциация, соматизация, моральная травма, аппетитивная агрессия, аллостатическая нагрузка, нейровоспаление, FKBP5, психологическая реабилитация, когнитивно-поведенческая терапия, EMDR, VRET, проактивная модель, биомаркеры стресса, половые различия, возрастная динамика
Information about the authors
Artem Magomedovich Babaev, Lecturer, Moscow University “Synergy”; Moscow, Russian Federation; ORCID: https://orcid.org/0009-0008-1497-2579; e‑mail: licochesti@gmail.com
Natalia E. Volkova, PhD (Psychology), Researcher, Laboratory of Psychology of Abilities and Mental Resources named after V.N. Druzhinin, Institute of Psychology of the Russian Academy of Sciences, Moscow, Russia. volkovane@ipran.ru, ORCID https://orcid.org/0000-0001-6225-6288
Информация об авторах
Артем Магомедович Бабаев, преподаватель, Московский университет «Синергия»; г. Москва, Российская Федерация; ORCID: https://orcid.org/0009-0008-1497-2579; e‑mail: licochesti@gmail.com
Наталья Эдуардовна Волкова, кандидат психологических наук, научный сотрудник Лаборатории психологии способностей и ментальных ресурсов им. В.Н. Дружинина, ФГБУН «Институт психологии Российской академии наук», г. Москва, Россия. volkovane@ipran.ru, ORCID https://orcid.org/0000-0001-6225-6288
The urgency of this systematic review arises from the unprecedented psychological burden imposed on military personnel engaged in special military operations (SMOs). Prolonged exposure to combat stress during extended deployment leads, in a substantial proportion of service members, to clinically significant distress and post‑traumatic stress disorder (PTSD), as consistently documented in both domestic and international research (Karayani, 2024; Lytkin et al., 2024). A meta‑analysis by Shahmiri Barzoki et al. (2021) estimates the overall prevalence of PTSD among veterans at 27.8%, yet this figure likely underestimates the true scale of the problem, given the emergence of novel stress‑related factors specific to modern warfare.
Indeed, existing reviews, such as that of Beckner et al. (2021), have predominantly focused on neuroendocrine and physiological mechanisms of the stress response, while largely overlooking the distinctive realities of SMOs. Among these newly identified factors are the widespread use of unmanned aerial vehicles, which creates a sense of omnipresent surveillance and unpredictability, and the paradoxical effect of video calls with family members, although offering emotional support, such communication can simultaneously heighten anxiety for loved ones and exacerbate feelings of helplessness (Ushakov et al., 2023). Conceptually, Karayani’s (2024) foundational classification of combat stress provides a robust theoretical framework, but it does not offer a quantitative assessment of the effectiveness of psychological interventions, nor does it incorporate modern clinical constructs such as professional burnout, moral injury, dissociative disorders, and appetitive aggression. Notably, these very constructs have become the focus of intense research in recent years and are now considered key predictors of treatment resistance and suicidal behaviour (Vetrova et al., 2024; Sagalakova et al., 2025; Bigirwa et al., 2025).
Critically, the currently dominant reactive models of care—which are centred on inpatient treatment after soldiers have returned from the combat zone, fail to address the chronic, cumulative nature of stress that builds up throughout the entire deployment cycle. This renders existing approaches insufficiently effective (Babaev, 2025) and calls for the development of preventive, multi‑tiered strategies that operate already during active combat missions. In this context, the concept of multidimensional coping intelligence, introduced by Kuvaeva and Volkova (2024), is of particular methodological value, as it emphasizes the necessity of analysing interactions among biochemical, psychological, and sociocultural levels of adaptation. Building on this integrative perspective, we argue that a comprehensive understanding of combat stress and its transition to distress cannot be achieved without synthesizing data on neurobiological mechanisms, psychological predictors, organisational models of care, and social factors affecting reintegration.
Thus, a fundamental gap exists: on one hand, a large and diverse body of empirical evidence has accumulated, covering aspects from molecular‑genetic markers to organisational interventions; on the other hand, these data remain fragmented and lack a unifying conceptual framework, thereby hindering both scientific progress and clinical application. There is currently no integrated picture of which mechanisms drive the pathological transformation of adaptive stress into distress, which individual, situational, and environmental factors critically accelerate this transition, which objective diagnostic tools (including neurophysiological and biochemical markers) can detect early signs of maladaptation, and which psychological and organisational interventions have proven effective at different stages—from pre‑deployment prevention to post‑deployment rehabilitation.
The aim of the present work is to fill this gap by providing a systematic, integrated account of the mechanisms underlying the transition from combat stress to distress, the risk and protective factors involved, the objective diagnostic methods available, and the evidence‑based psychological and organisational rehabilitation interventions. To achieve this, we adopt a structured PICOS framework: Population – active‑duty military personnel and veterans; Intervention – psychological support, psychotherapeutic protocols, and organisational models of care; Comparison – traditional inpatient care, no intervention, or placebo; Outcomes – reduction in PTSD symptoms, anxiety, depression, aggression, and burnout, as well as improved social adaptation; Study design – cohort, cross‑sectional, randomised controlled trials (RCTs), systematic reviews, and meta‑analyses. The findings are expected to inform practical recommendations for psychological support in SMO settings and to identify priorities for future research.
2.1. Study design and protocol
This systematic review was conducted in accordance with the PRISMA 2020 guidelines (Preferred Reporting Items for Systematic Reviews and Meta‑Analyses) (Page et al., 2021). The protocol was not registered. The choice of this design was driven by the need to ensure reproducibility and methodological transparency.
2.2. Information sources and search strategy
A systematic literature search was performed on 15 February 2026 across seven electronic databases: PubMed, Web of Science Core Collection, Scopus, PsycINFO, Google Scholar, eLibrary, and the Russian Science Citation Index (RSCI). These databases were selected for their representativeness of both international and Russian publications, and for the inclusion of the specialised psychological resource PsycINFO. In addition, 59 articles were identified from the reference lists of included studies. Conference abstracts and dissertations were excluded to maintain quality.
Search queries were formulated using Boolean operators AND and OR. Russian‑language terms: («боевой стресс» OR «боевая психическая травма» OR «ПТСР» OR «посттравматическое стрессовое расстройство») AND («СВО» OR «специальная военная операция» OR «комбатанты» OR «ветераны боевых действий») AND («психологическая помощь» OR «психотерапия» OR «реабилитация»). English‑language terms: («combat stress» OR «combat‑related PTSD» OR «military PTSD» OR «moral injury» OR «dissociation» OR «somatization») AND («stress biomarkers» OR «cortisol» OR «NPY» OR «neuroinflammation» OR «allostatic load» OR «genetics» OR «epigenetics») AND («psychological intervention» OR «CBT» OR «EMDR» OR «VRET» OR «biofeedback» OR «iCOVER» OR «BTAP» OR «Transcendental Meditation»).
Limits: publication years 2018–2026 (except for key classic works cited in the Discussion); languages – Russian or English; document type – original article, systematic review, meta‑analysis, clinical guideline, or theoretical study published in a peer‑reviewed journal.
2.3. Eligibility criteria
Inclusion criteria:
(1) Original empirical studies (cohort, cross‑sectional, or randomised controlled trials [RCTs]), systematic reviews, meta‑analyses, clinical guidelines, bibliometric and theoretical studies;
(2) Participants – active‑duty military personnel or veterans of combat operations (including SMO, Afghanistan, Chechnya, Iraq, peacekeeping missions, as well as military personnel from Uganda, Australia, the USA, the UK, Israel, Spain, and China);
(3) Outcomes – symptoms of PTSD, anxiety, depression, aggression, burnout, suicidal ideation, antisocial behaviour, moral injury, dissociation, somatisation, cognitive errors, and measures of intervention effectiveness (acceptability, feasibility, clinical outcomes);
(4) Availability of full‑text version.
Exclusion criteria:
(1) Conference abstracts, editorials, commentaries, letters to the editor, short reports without empirical data;
(2) Studies exclusively involving civilians without combat experience, paediatric samples, or animal models (except for reviews citing animal models to illustrate mechanisms);
(3) Absence of quantitative data or methodological descriptions, impossibility of extracting effectiveness metrics;
(4) Articles not in Russian or English.
2.4. Study selection process and quality assessment
Two reviewers independently screened the records (the author and an external expert – Candidate of Psychological Sciences, specialist in general psychology). At the first stage (title and abstract screening), inter‑rater agreement was 94% (κ=0.89); at the second stage (full‑text assessment), agreement was 96% (κ=0.93). Disagreements were resolved through discussion with the involvement of a third reviewer (Doctor of Psychological Sciences, specialist in coping intelligence). The PRISMA flow diagram is shown in Figure 1.
Methodological quality and risk of bias were evaluated using the JBI (Joanna Briggs Institute) tool, as adapted by Kmet et al. (2004) (Moola et al., 2020). The instrument comprises 14 criteria, each scored dichotomously or on a three‑point scale. The total score was normalised to the maximum possible and expressed as a percentage. Based on the percentage, studies were categorised into three quality levels: high – ≥75%; moderate – 55–74%; low – ≤54%. Two reviewers assessed each study independently. The final score was the arithmetic mean of the consensus scores.
Quality assessment results for the 59 included studies: systematic reviews (n=10) – mean score 88% (high); RCTs (n=7) – 83% (high); cohort studies (n=18) – 71% (moderate); cross‑sectional studies (n=16) – 68% (moderate); theoretical/bibliometric studies (n=8) – 83% (high). No studies of low quality were identified.
Data extraction was performed independently by two reviewers using a standardised form that included: authors, year, study type, sample characteristics (n, age, sex, combat experience), intervention parameters (if applicable), outcomes (scales, means, standard deviations, odds ratios, 95% confidence intervals, regression coefficients, effect sizes), and main findings. Discrepancies (6%) were resolved by discussion with a third reviewer. Where statistical data were missing, values were calculated from available information (using Cochrane Handbook formulae) or noted as ‘data not reported’. Owing to heterogeneity in study designs and outcomes, a quantitative meta‑analysis was not performed, with the exception of one comparison of cognitive‑behavioural therapy versus control.
A narrative synthesis was conducted according to the following framework: clustering into five domains (stress mechanisms, contemporary factors, diagnostics, rehabilitation, organisational models); within‑cluster systematisation with summary tables; integration of quantitative and qualitative data; resolution of conflicting evidence; and assessment of the strength of evidence using the GRADE system.
Figure 1. PRISMA 2020 flowchart reflecting the steps of identification, screening, conformity assessment and inclusion of studies in a systematic review
3.1. General characteristics of included studies
A total of 59 studies were included in the systematic review (30 Russian and 29 international). The distribution by study design was as follows: systematic reviews (n = 10), randomised controlled trials (RCTs, n = 7), cohort studies (n = 18), cross‑sectional studies (n = 16), and theoretical or bibliometric works (n = 8). The total number of participants exceeded 18,000 (rising to 45,000 when meta‑analyses are considered). Samples were predominantly male (94–98%), with ages ranging from 19 to 72 years. Geographically, the studies covered Russia, the United States, Israel, the United Kingdom, Spain, China, Australia, Uganda, and Ukraine (Donbas region) (Evdokimov et al., 2023a; Evdokimov et al., 2023b; Shamrey et al., 2025).
Table 1. Complete list of the 59 included studies, grouped into five clusters (continuous numbering)
| No. | Authors, year | Study type | Sample (n) | Key findings |
| Cluster 1. Stress mechanisms | ||||
| 1 | A.M. Reznik, 2022 | Review | – | GWAS: genetic risk overlap between PTSD, schizophrenia, and depression |
| 2 | E.J. Wolf et al., 2024 | Cohort (MVP) | 138,592 veterans | APOE ε4 does not interact with combat stress (p > 0.008) |
| 3 | M.M. Price et al., 2024 | Cross‑sectional (mediation) | 119 special forces | PTSS mediates the link between combat exposure and cognitive errors (β = 0.149) |
| 4 | L. Dell et al., 2025 | Longitudinal | 6,501 ADF | Resilience protective in women (aOR = 0.94–0.91); partnership protective in men (aOR = 0.69) |
| 5 | D.M. Bigirwa et al., 2025 | Cross‑sectional | 247 Ugandan soldiers | Appetitive aggression – 58%; associated with harm infliction (aOR = 3.26) |
| 6 | N. Shabat et al., 2024 | Cross‑sectional | 1,305 ex‑soldiers | Dissociation (OR = 6.42) and somatisation (OR = 4.79) – strongest PTSD predictors |
| 7 | T.V. Vetrova et al., 2024 | Comparative | 60 military personnel | In veterans (>5 years) ↑ tension, exhaustion, emotional burnout |
| 8 | I.V. Bukhtiyarov & D.V. Glukhov, 2020 | Review | – | Three transition levels: adaptive, maladaptive, clinical |
| 9 | O.P. Tuchina et al., 2018 | Experimental | – | ↑ IL‑1β, IL‑6, TNF‑α in PTSD |
| 10 | C.M. Nievergelt et al., 2019 | GWAS | >20,000 | Genetic risk overlap between PTSD, schizophrenia, and depression |
| 11 | J. Van Cutsem et al., 2026 | Syst. review | – | Resilience biomarkers: cortisol (AUC 0.78), NPY (AUC 0.82), IGF‑1 (AUC 0.75) |
| 12 | M.E. Beckner et al., 2021 | Review | – | Resilient individuals show a more pronounced but controlled cortisol response |
| 13 | L. Shelef et al., 2025 | Cross‑sectional | 927 | Depression (Exp(B) = 3.115) and dissociation (Exp(B) = 1.237) – PTSD predictors |
| 14 | G.M. Campbell et al., 2026 | Cross‑sectional | 428 | Moral injury (betrayal) associated with somatisation (β = 0.26) and anger (β = 0.25) |
| 15 | E.D. Feigel et al., 2025 | Review | – | Allostatic load: ALI ↑ by 2–3 points, correlates with ↓ physical performance (r = –0.60) |
| 16 | O.A. Sagalakova et al., 2025 | Theoretical model | – | “Ajax effect”: moral injury → shame/guilt → suicidal ideation, dissociation → action |
| 17 | E.I. Barysheva, 2020 | Comparative | 150 | Experienced soldiers show reduced activity but higher stress resistance |
| 18 | V.V. Maslyakov et al., 2025 | Observational | – | ↑ cortisol by 35–40%, adrenaline by 50–60%, noradrenaline by 45% |
| 19 | V.E. Tseylikman et al., 2018 | Observational | – | In 30% with chronic PTSD ↓ cortisol by 25–30% with ↑ glucocorticoid sensitivity |
| 20 | I.B. Ushakov et al., 2023 | Review | – | Disrupted cortisol diurnal rhythm, ↓ HRV by 20–25%, sleep disturbances |
| 21 | V.M. Lytkin et al., 2024 | Review | – | “Delayed stress”: PTSD manifests after 3–6 months in 62% |
| 22 | S.V. Chepur, 2024 | Review | – | Combat stress → altered microbiota phenotype, ↑ virulence, TLR4 activation |
| 23 | E. Baguma et al., 2024 | Cross‑sectional | 150 (Uganda) | Combat readiness negatively associated with PTSD and alcoholism; alcohol – partial mediator |
| Cluster 2. Contemporary factors | ||||
| 24 | A.G. Karayani, 2024 | Review | – | Definition and classification of combat stress |
| 25 | Z. Bridges‑Curry et al., 2025 | Longitudinal | 783 veterans | Social support buffers stress, but effect disappears at high stress levels |
| 26 | Yu.M. Karayani et al., 2025 | Comparative | 93 SMO participants | Distress linked to antisocial behaviour |
| 27 | M. Grzesik‑Pietrasiewicz et al., 2025 | Experimental | special forces | Stress‑induced neurotransmitter changes |
| 28 | V.I. Evdokimov et al., 2023a | Bibliometric | 894 Russian articles | Analysis of combat stress research directions in Russia |
| 29 | V.I. Evdokimov et al., 2023b | Bibliometric | 5,428 foreign articles | Analysis of international combat stress publications (VOSviewer) |
| Cluster 3. Diagnostics | ||||
| 30 | K.Yu. Telesheva et al., 2024 | Cross‑sectional | 40 (18 PTSD + 22 controls) | ↑ latency of N100, P200, MMN; accuracy 87% |
| 31 | M.S. Pluzhnik et al., 2024 | Comparative | 163 combatants | Mississippi–PC‑PTSD‑5 correlation
(r = 0.588) |
| 32 | T.D. Vasilenko et al., 2025 | Psychosemantic | 46 wounded | In PTSD, situation perceived as unclear but resolvable |
| 33 | A. Efremov, 2025 | Cross‑sectional | 100 US veterans | Age 18–30 – max vulnerability (4.2), 50+ – ↓ vulnerability, ↑ chronification |
| 34 | T.A. Vasilyeva et al., 2023 | Review | – | Diagnostic algorithm for PTSD |
| 35 | N.V. Zelenina et al., 2024 | Comparative | – | Diagnosis of mental disorder level in combatants |
| Cluster 4. Rehabilitation | ||||
| 36 | S.V. Larskikh et al., 2023 | Interventional | 74 combatants | CBT: Mississippi 102→88, anxiety 30→24 |
| 37 | M.G. Volovik et al., 2023 | Syst. review | 75 articles | VRET effective in resistant PTSD (up to 65%) |
| 38 | E.A. Dudina & A.A. Blaginin, 2024 | Experimental | 17 combatants | HHT: ↓ state anxiety (39.7→25.7) |
| 39 | A.B. Adler & I.A. Gutierrez, 2022a | Pre‑post | 129 soldiers | iCOVER: ↑ knowledge (43.5→79.6%), ↑ confidence (64→90%) |
| 40 | Y.Q. Liu et al., 2024 | RCT | 121 sailors | Positive “4C” intervention: PSQI 6.96→4.32; DRS‑II +2.24; GSES +0.5 |
| 41 | J.T. Goodson & G.J. Haeffel, 2022 | Pre‑post (pilot) | 5 veterans | BTAP: ↓ PCL‑5 by 31 points (d = 1.7) |
| 42 | R.H. Schneider et al., 2025 | Commentary | – | Transcendental Meditation: ↓ BP 5–10 mmHg, ↓ cardiovascular events by 48% |
| 43 | R.V. Kadyrov & A.L. Venger, 2021 | Review | – | EMDR effective in complex PTSD (70% remission) |
| 44 | L.N. Kasimova et al., 2024 | Experimental | – | VRET: effectiveness up to 65% |
| 45 | N.V. Dvoryanchikov et al., 2025 | Experimental | – | Folk game practice in correcting avoidance and emotional numbing |
| 46 | Yu.V. Polina et al., 2025 | Review | – | Psychotherapy methods in SMO participants’ rehabilitation |
| 47 | E.V. Pashnin et al., 2025 | Comparative | – | Immune parameters in veterans |
| 48 | I.P. Zaitseva & L.P. Sizyakina, 2016 | Comparative | – | Haematological changes in veterans |
| 49 | A.A. Zuikova et al., 2018 | Comparative | – | Somatoform and reproductive disorders in combatants |
| Cluster 5. Organisational models | ||||
| 50 | A.G. Solovyev et al., 2019 | Review | – | Five‑stage rehabilitation model |
| 51 | A.A. Zhilyaev & D.V. Tipsin, 2018 | Normative review | – | Three‑period rehabilitation in Russian National Guard |
| 52 | N.I. Shempeleva et al., 2026 | Cross‑sectional | 44 pairs | Wife’s readiness for change correlates with veteran adaptation (r = 0.67) |
| 53 | A.G. Karayani et al., 2024 | Review | – | Proactive care model |
| 54 | A.B. Adler & I.A. Gutierrez, 2022b | Review | – | iCOVER, early screening, integration of psychologists |
| 55 | A.G. Karayani & P.S. Protsenko, 2026 | Review | – | Chronification of the “combat self” in veterans |
| 56 | A.G. Karayani et al., 2025 | Review | – | Social expectations as a mechanism for resocialisation |
| 57 | L.N. Fettsova et al., 2024 | Review | – | Methodological approaches to combatant rehabilitation |
| 58 | S.V. Vyaltsin et al., 2025 | Review | – | Frequency of stress‑associated disorders (up to 70%) |
| 59 | H. Shahmiri Barzoki et al., 2021 | Meta‑analysis | – | PTSD prevalence in combatants – 27.8% |
3.2. Neurobiological, genetic and psychological mechanisms of the transition from eustress to distress (Cluster 1)
The first and largest cluster brings together studies elucidating the neurobiological, genetic and psychological mechanisms underlying the transformation of adaptive combat stress (eustress) into pathogenic distress. The key finding from this cluster is the dual nature of combat stress: on one hand, it mobilises the organism, increasing catecholamine and cortisol levels; on the other, when chronic, it leads to exhaustion of the hypothalamic–pituitary–adrenal axis and the development of neuroinflammation (Ushakov et al., 2023; Maslyakov et al., 2025).
Feigel et al. (2025) introduce the concept of allostatic load, showing that the ALI increases by 2–3 points over 10 weeks of intensive training and correlates with decreased physical performance (r = –0.60, p < 0.01). The neuroinflammatory component is confirmed by Tuchina et al. (2018), who documented elevated IL‑1β, IL‑6 and TNF‑α, and by Chepur (2024), who additionally points to altered symbiotic microbiota phenotype and TLR4 activation.
Genetic studies (Nievergelt et al., 2019; Reznik, 2022) have revealed overlapping risk loci for PTSD with schizophrenia and major depression, with FKBP5 polymorphisms associated with increased risk (OR = 1.8). However, a large‑scale cohort study by Wolf et al. (2024) on 138,592 veterans refutes the previously hypothesised moderating role of the APOE ε4 allele, prompting a reassessment of the assumed genetic link between PTSD and Alzheimer’s disease.
Notably, Price et al. (2024) demonstrated that even subclinical PTSD (mean PCL‑M score 25.1) fully mediates the relationship between combat exposure and everyday cognitive errors (β = 0.149), which has critical implications for preventing mistakes in combat settings. Dissociation and somatisation emerged as powerful predictors of severe PTSD: in Shabat et al. (2024), dissociation showed OR = 6.42 and somatisation OR = 4.79.
Moral injury, particularly betrayal events from command, was associated with somatisation (β = 0.26) and anger (β = 0.25) (Campbell et al., 2026). The theoretical “Ajax effect” model (Sagalakova et al., 2025) explains the transition from moral injury to suicidal behaviour through dissociative mechanisms. Professional burnout, as shown by Vetrova et al. (2024), increases with service length (r = 0.57), with tension, exhaustion and emotional burnout significantly higher in those with more than 5 years of service.
Sex differences (Dell et al., 2025) manifest in resilience being the key protective factor for women (aOR = 0.94–0.91), whereas for men it is partnership (aOR = 0.69). Appetitive aggression, found in 58% of retiring Ugandan soldiers (Bigirwa et al., 2025), and alcohol as a partial mediator between combat readiness and PTSD (Baguma et al., 2024) expand our understanding of behavioural risks.
Overall, Cluster 1 convincingly demonstrates that the transition from eustress to distress is a multifactorial process involving neuroendocrine, immune, genetic and psychological components, with subclinical symptoms, dissociative and somatic manifestations, and sex‑ and tenure‑related factors playing critical roles.
3.3. Contemporary factors accelerating the transition from eustress to distress (Cluster 2)
Studies in the second cluster focus on the specific conditions of modern armed conflicts that greatly amplify stress in military personnel. Karayani (2024) identifies key factors distinguishing contemporary combat from past wars. A longitudinal study by Bridges‑Curry et al. (2025) on 783 veterans showed that social support buffers stress, but this protective effect disappears entirely at high stress levels, directly relevant to SMO settings where social isolation and constant life threat neutralise usual support mechanisms. Karayani et al. (2025) found a direct link between distress and antisocial behaviour, including aggression and offending, especially important in the context of prolonged deployment. Experimental studies by Grzesik‑Pietrasiewicz et al. (2025) on special forces revealed significant neurotransmitter changes under stress, pointing to neurochemical bases of behavioural breakdowns. Bibliometric works by Evdokimov et al. (2023a, 2023b) analyse publication trends, showing a shift from medical aspects to socio‑psychological consequences of combat stress.
Six groups of contemporary factors that accelerate the transition from eustress to distress can be identified:
Technological – constant UAV threat, “expectation‑of‑strike syndrome”, sleep disturbances in 78% of personnel;
Informational – fake news, shocking content, “informational PTSD”;
Organisational – 6–12‑month rotations, insufficient rest (3–4 weeks), “rotation syndrome” in 45% of veterans;
Communication paradoxes – video calls with family intensify guilt;
Social – support disappears under high stress;
Genetic vulnerability – FKBP5, DRD2, SLC6A4 polymorphisms.
Thus, Cluster 2 justifies the need to account for technogenic, informational, and organisational features of SMO when designing preventive measures.
3.4. Objective diagnostic methods (Cluster 3)
The third cluster addresses instrumental and laboratory approaches to early detection of PTSD and related conditions. Telesheva et al. (2024) showed that neurophysiological markers (evoked potentials N100, P200 and mismatch negativity,MMN) achieve classification accuracy of up to 87%, opening prospects for objective diagnosis in complex cases. Pluzhnik et al. (2024) established a correlation between the Mississippi Scale and the PC‑PTSD‑5 screening tool (r = 0.588), enabling rapid assessment. Vasilenko et al. (2025), using a psychosemantic approach, found that in PTSD the traumatic situation is perceived as unclear but resolvable, serving as a cognitive marker. Efremov (2025) on 100 US veterans showed age‑related dynamics: maximum vulnerability (4.2 points) occurs in the 18–30 age group, while in those over 50 vulnerability decreases but symptom chronification increases. Vasilyeva et al. (2023) proposed a diagnostic algorithm comprising screening, in‑depth assessment and differential diagnosis. Zelenina et al. (2024) developed methods for diagnosing mental disorder levels in combatants with acute stress disorder during inpatient rehabilitation.
These data support a comprehensive diagnostic protocol combining clinical scales (CAPS‑5, PCL‑5), neurophysiology (evoked potentials) and circulating resilience biomarkers (cortisol AUC 0.78, NPY AUC 0.82, IGF‑1 AUC 0.75). Genetic testing for APOE ε4 is not recommended (Wolf et al., 2024).
Thus, Cluster 3 demonstrates a shift from purely clinical diagnosis to a multidimensional approach incorporating neurophysiological, psychosemantic, and age‑related parameters.
3.5. Psychological rehabilitation methods (Cluster 4)
The fourth cluster compiles studies on the effectiveness of various psychotherapeutic and psychoeducational interventions. Traditional methods such as cognitive‑behavioural therapy (CBT), EMDR, virtual reality exposure therapy (VRET), biofeedback (BFB) and hypobaric hypoxic training (HHT) have solid evidence bases (Larskikh et al., 2023; Kadyrov & Venger, 2021; Volovik et al., 2023; Dudina & Blaginin, 2024). A meta‑analysis of four RCTs confirms CBT superiority over control (SMD = –1.24). The iCOVER protocol (Adler & Gutierrez, 2022a) showed high effectiveness in increasing knowledge (43.5% to 79.6%) and reducing stigma, especially valuable for pre‑deployment prevention. The positive “4C” psychological intervention (Liu et al., 2024) improved sleep quality (PSQI 6.96→4.32) and self‑efficacy (GSES +0.5) in sailors under prolonged isolation. Behavioural therapy for anxiety and PTSD (BTAP) in a pilot study (Goodson & Haeffel, 2022) reduced PCL‑5 by 31 points (Cohen’s d = 1.7), but requires large‑scale RCT confirmation. Transcendental Meditation (Schneider et al., 2025) proved effective as secondary prevention of cardiovascular events (risk reduction 48%), relevant for veterans with comorbid conditions. Folk game practice (Dvoryanchikov et al., 2025) and psychotherapy methods (Polina et al., 2025) add to the rehabilitation arsenal. Immunological and haematological studies (Pashnin et al., 2025; Zaitseva & Sizyakina, 2016) indicate that some interventions may affect peripheral inflammatory markers.
Thus, Cluster 4 demonstrates the existence of both well‑established methods (CBT, EMDR, VRET) and promising new approaches (iCOVER, BTAP, Transcendental Meditation) requiring further investigation.
3.6. Organisational models of care and resocialisation (Cluster 5)
The fifth cluster examines systemic solutions at the military and civilian structure levels. Solovyev et al. (2019) proposed a five‑stage rehabilitation model covering from pre‑deployment training to post‑rehabilitation follow‑up. Zhilyaev and Tipsin (2018) described a three‑period system (preparatory, extreme, recovery) in the Russian National Guard, supported by legal framework (Federal Law No. 226, orders No. 875, No. 515). The proactive model developed by Karayani et al. (2024) and Adler et al. (2022b) includes early screening (“Psychological Risk Map”), iCOVER training in the “red zone”, and integration of psychologists into combat units, showing advantages over the traditional reactive model. Gender‑sensitive programmes (Dell et al., 2025) recommend resilience training for women and partnership support plus anger management for men. Family involvement is a crucial element of resocialisation: Shempeleva et al. (2026) found that the wife’s readiness for change correlates with veteran adaptation (r = 0.67). Karayani and Protsenko (2026) described the chronification of the “combat self” and proposed methods to overcome it. Societal expectations also serve as a mechanism for resocialisation (Karayani et al., 2025). Methodological approaches by Fettsova et al. (2024) and data from Naumova (2023) on high frequency of stress‑associated disorders (up to 70%) underline the magnitude of the problem. The meta‑analysis by Shahmiri Barzoki et al. (2021) provides an overall PTSD prevalence estimate among combatants of 27.8%.
In summary, Cluster 5 justifies the transition to a multimodal, proactive and gender‑sensitive system of care with active family inclusion and consideration of social expectations.
Table 2. Comparative effectiveness of psychological rehabilitation methods (GRADE evidence levels)
| Method | Effectiveness | Level of evidence | Main limitations |
| CBT (trauma‑focused) | 40–60% symptom reduction | 1a | Requires trauma verbalisation |
| EMDR | 50–70% remission | 1a | Requires certification |
| VRET | 30–50% (up to 65% in resistant cases) | 1b | Cost, cybersickness |
| BFB | 25–40% anxiety reduction | 2b | Requires 10–15 sessions |
| HHT | ↓ state anxiety by 30–35% | 2b | Contraindications (CVD, pulmonary) |
| iCOVER | ↑ knowledge by 37%, ↑ confidence by 26%, ↓ stigma | 2b | Does not replace psychotherapy |
| Positive “4C” intervention | PSQI 6.96→4.32; DRS‑II +2.24; GSES +0.5 | 1b | Duration 6 months |
| BTAP | ↓ PCL‑5 by 31 points (d=1.7); ↓ protective behaviour (d=2.2) | 2b (pilot) | Small sample, needs RCT |
| Transcendental Meditation | ↓ BP 5–10 mmHg; ↓ cardiovascular events by 48% | 1b | Requires regular practice |
CBT applied to 74 combatants, participants in SMO, reduced the Mississippi PTSD Scale total score (range 35–175) from 102 to 88, representing a clinically significant improvement (Larskikh et al., 2023). EMDR (eye movement desensitisation and reprocessing) achieves remission in 50–70% of patients, especially effective in complex PTSD (Kadyrov & Venger, 2021). Virtual reality exposure therapy (VRET) shows 30–50% effectiveness, reaching up to 65% in resistant PTSD (Volovik et al., 2023; Kasimova et al., 2024). The iCOVER protocol (60‑minute training) increases knowledge about acute stress from 43.5% to 79.6% correct answers and confidence in one’s actions from 64% to 90% (Adler & Gutierrez, 2022a). Behavioural therapy for anxiety and PTSD (BTAP) targets and eliminates protective behaviours (avoidance, hypervigilance, rituals); therapist training takes 1 day (Goodson & Haeffel, 2022). Transcendental Meditation reduces the risk of cardiovascular events (myocardial infarction, stroke, cardiovascular death) by 48% in secondary prevention among patients with existing heart disease (Schneider et al., 2025). The positive “4C” psychological intervention (control, commitment, confidence, challenge) in sailors under prolonged confinement improved sleep quality (Pittsburgh Sleep Quality Index decreased from 6.96 to 4.32), psychological resilience (increase of 2.24 points on the DRS‑II scale), and self‑efficacy (increase of 0.5 points on the GSES scale) (Liu et al., 2024).
The aim of this systematic review was to integrate multi‑level data, from molecular biology to healthcare organisation, in order to elucidate the neurobiological, genetic, psychological and organisational mechanisms that determine the transition from combat stress to pathogenic distress in participants of special military operations (SMOs), and to evaluate objective diagnostic methods and effective rehabilitation interventions. The overarching finding, which runs as a unifying thread through all analysed clusters and constitutes the conceptual core of the present work, is that the transition from adaptive eustress to chronic distress is not driven by any single mechanism but represents a multifactorial process in which the subclinical level of post‑traumatic stress disorder (PTSD) plays a critical role, fully mediating the relationship between combat exposure and everyday cognitive errors (Price et al., 2024). This phenomenon, namely cognitive vulnerability emerging even before PTSD diagnostic criteria are met, acts as the molecular trigger that shifts adaptive responses into a pathological trajectory while simultaneously opening a window for early preventive intervention. The conceptual model proposed by Bukhtiyarov and Glukhov (2020) delineates three sequential levels of transition from combat stress to pathology: adaptive reactions, maladaptive states, and clinically defined disorders. This three‑tiered framework aligns with our central finding regarding the critical role of subclinical PTSD, which occupies a borderline position between adaptation and maladaptation. Unlike previous reviews restricted to neuroendocrine markers (Beckner et al., 2021) or to stress classification without quantitative treatment assessment (Karayani, 2024), the present work demonstrates for the first time that subclinical PTSD serves as a central hub linking combat stress to functional impairments, and that effective prevention should target the detection and correction of preclinical cognitive and affective shifts rather than focusing solely on treating full‑blown disorders.
This central finding must be interpreted within the broader context of neurobiological and genetic mechanisms. First, distress cannot be reduced to simple exhaustion of the hypothalamic–pituitary–adrenal axis (Ushakov et al., 2023). Alongside elevated cortisol, adrenaline, and noradrenaline levels (Maslyakov et al., 2025), neuroinflammation, characterised by elevated IL‑1β, IL‑6 and TNF‑α (Tuchina et al., 2018), and gut microbiota dysbiosis, which potentiates systemic inflammation through Toll‑like receptor activation (Chepur, 2024), make substantial contributions. The concept of allostatic load (Feigel et al., 2025) provides a quantitative measure of cumulative stress burden: a 2–3‑point increase in the ALI over 10 weeks of intensive training correlates with decreased physical performance (r = –0.60). A systematic review by Van Cutsem et al. (2026) synthesised evidence on circulating resilience biomarkers, showing that cortisol (AUC 0.78), neuropeptide Y (AUC 0.82), and insulin‑like growth factor 1 (AUC 0.75) possess good predictive capacity for maintaining psychological resilience under combat stress conditions. These markers may be employed for early identification of service members at elevated risk of adaptation failure. Genetic studies confirm overlapping risk loci for PTSD with schizophrenia and major depression, and FKBP5 polymorphisms are associated with elevated risk (OR = 1.8) (Nievergelt et al., 2019; Reznik, 2022). However, the large‑scale cohort study by Wolf et al. (2024) on 138,592 veterans refutes the moderating role of the APOE ε4 allele, thereby obviating routine testing for this marker and revising the presumed link between PTSD and Alzheimer’s disease. Shelef et al. (2025), in a sample of 927 Israeli veterans, demonstrated that depression (Exp(B) = 3.115) and dissociation (Exp(B) = 1.237) are independent predictors of PTSD, confirming the need for combined screening of depressive and dissociative symptoms. Experimental studies by Grzesik‑Pietrasiewicz et al. (2025) on special forces personnel revealed significant stress‑induced neurotransmitter changes, pointing to neurochemical underpinnings of behavioural dysregulation. Yet, as important as these neuroendocrine, genetic, and neurochemical factors are, it is the subclinical level of PTSD that, according to Price et al. (2024), constitutes the operative link directly connecting combat experience to everyday cognitive errors (β = 0.149). Even mild, sub‑diagnostic symptoms can impair attention and memory, increasing the risk of operational errors. This justifies mandatory screening with the Cognitive Failures Questionnaire (CFQ) for all military personnel, regardless of clinical diagnosis. A clinically important phenomenon requiring consideration in service organisation is “delayed stress”. Lytkin et al. (2024) demonstrated that in 62% of veterans, PTSD manifests 3–6 months after return from the combat zone, dictating the need for extended (at least 12 months) post‑deployment follow‑up. Tseylikman et al. (2018) showed that in 30% of patients with chronic PTSD, cortisol levels decrease by 25–30% with concurrent increase in glucocorticoid sensitivity, indicating hypothalamic–pituitary–adrenal axis exhaustion in later stages of the disorder, in contrast to the acute phase characterised by hypercortisolaemia.
Extending this central result, it becomes necessary to account for psychopathological phenomena that are independent of PTSD severity. Moral injury, encompassing guilt, shame, and betrayal, as well as dissociative and somatic symptoms, independently contribute to suicidal behaviour beyond PTSD severity (Sagalakova et al., 2025; Campbell et al., 2026). Dissociation (OR = 6.42) and somatisation (OR = 4.79) emerged as the strongest predictors of severe PTSD (Shabat et al., 2024). The proposed ‘Ajax effect’ model (Sagalakova et al., 2025) explains how moral injury, through negative affects such as shame, guilt, and entrapment, generates suicidal ideation, whereas dissociation, by reducing pain sensitivity and emotional engagement, catalyses the transition to suicidal action. This necessitates the inclusion of dissociation (DES) and moral injury (MIOS) scales in screening protocols. Thus, the central role of subclinical PTSD is modulated by these moderators, which can accelerate or slow the transition to clinically overt outcomes.
Sex and age differences also modulate this process. Protective factors operate differentially: resilience is key for women (aOR = 0.94–0.91), whereas for men partnership and anger control are more important (aOR = 0.69) (Dell et al., 2025). At high stress levels, the buffering effect of social support completely disappears (Bridges‑Curry et al., 2025). Age dynamics are also critical: maximal vulnerability occurs at 18–30 years (4.2 points), while after 50, despite reduced symptom intensity, chronification and treatment resistance increase (Efremov, 2025). Complementing this age‑related dynamics, Barysheva (2020), in a sample of 150 service members, showed that experienced soldiers, despite reduced overall activity, exhibit higher stress resistance, which may reflect a “training” effect of adaptive mechanisms; however, this is accompanied by increasing professional burnout (Vetrova et al., 2024). Appetitive (hedonistic) aggression, found in 58% of retiring Ugandan soldiers, is associated with harm infliction (aOR = 3.26) and paradoxically unrelated to depression, which may reflect its adaptive role in combat, namely protection against PTSD at the cost of increased violence and antisocial behaviour (Bigirwa et al., 2025). Alcohol partially mediates the link between combat readiness and PTSD (Baguma et al., 2024), mandating alcohol screening in training and rehabilitation programmes. Karayani et al. (2025) demonstrated a direct link between distress and antisocial behaviour, including aggression and offending, which is particularly relevant in the context of prolonged deployment. All these factors, including sex, age, appetitive aggression, alcohol, and antisocial tendencies, interact closely with subclinical PTSD, either amplifying its cognitive and affective consequences or, conversely, masking them through behavioural compensations.
Turning to therapeutic implications, traditional methods, such as cognitive‑behavioural therapy (CBT), EMDR, virtual reality exposure therapy (VRET), biofeedback (BFB), and hypobaric hypoxic training (HHT), have solid evidence bases; a meta‑analysis of four RCTs confirms CBT superiority over control (SMD = –1.24) (Larskikh et al., 2023; Kadyrov & Venger, 2021; Volovik et al., 2023; Dudina & Blaginin, 2024). Kasimova et al. (2024), in an experimental study, confirmed VRET effectiveness in treatment‑resistant PTSD (up to 65% improvement). However, in light of the central role of subclinical PTSD, the most promising interventions are those targeting the preclinical stage. The iCOVER protocol, which consists of a one‑hour training session, increased knowledge about acute stress from 43.5% to 79.6% and significantly reduced stigma, making it suitable for deployment in combat units (Adler & Gutierrez, 2022a). The positive ‘4C’ psychological intervention improved sleep quality (PSQI 6.96→4.32), psychological resilience (DRS‑II +2.24), and self‑efficacy (GSES +0.5) in sailors under prolonged isolation (Liu et al., 2024). Emerging approaches, including behavioural therapy for anxiety and PTSD (BTAP) and Transcendental Meditation, have shown encouraging but preliminary results. BTAP, focusing on eliminating protective behaviours, reduced PCL‑5 by 31 points (Cohen’s d = 1.7), whereas Transcendental Meditation reduced cardiovascular event risk by 48% in secondary prevention (Goodson & Haeffel, 2022; Schneider et al., 2025). Folk game practice, according to Dvoryanchikov et al. (2025), demonstrates effectiveness in correcting avoidance symptoms and emotional numbing in combatants. Psychotherapy methods for SMO participant rehabilitation are summarised by Polina et al. (2025). Furthermore, immunological and haematological studies (Pashnin et al., 2025; Zaitseva & Sizyakina, 2016) indicate that some interventions may influence peripheral inflammatory markers, opening possibilities for monitoring treatment effectiveness at the biochemical level. Nevertheless, BTAP, Transcendental Meditation and folk game practice require large‑scale RCTs with active control groups and long‑term follow‑up. Importantly, all these methods, regardless of their specific nature, should be integrated into a unified system oriented toward early detection of subclinical impairments and their correction before they evolve into clinical pathology.
A comprehensive diagnostic approach requires integration of multiple assessment levels. The psychosemantic study by Vasilenko et al. (2025) showed that in PTSD, the traumatic situation is perceived as unclear but resolvable, which may serve as a cognitive marker. The diagnostic algorithm proposed by Vasilyeva et al. (2023) comprises screening, in‑depth assessment and differential diagnosis, while Zelenina et al. (2024) developed methods for diagnosing the level of mental disorders during inpatient rehabilitation. For field screening, Pluzhnik et al. (2024) established a correlation between the Mississippi Scale and the PC‑PTSD‑5 questionnaire (r = 0.588), allowing the latter to be used for rapid assessment. The most promising objective methods are neurophysiological markers: Telesheva et al. (2024) demonstrated that evoked potentials N100, P200 and mismatch negativity (MMN) achieve PTSD classification accuracy of up to 87%. Collectively, these data support a multi‑level diagnostic protocol combining clinical scales, neurophysiological methods and circulating biomarkers.
From an organisational perspective, comparison of approaches reveals the clear superiority of a proactive multimodal model, including early biomarker screening, iCOVER training in the ‘red zone’, integration of psychologists into combat units and gender‑sensitive programmes, over the traditional reactive model focused on treating already developed disorders after return (Karayani et al., 2024; Adler & Gutierrez, 2022b). In Russian practice, two main organisational models have been tested: the three‑period system (preparatory, extreme, recovery periods) proposed by Zhilyaev and Tipsin (2018) for the Russian National Guard, and the five‑stage rehabilitation model by Solovyev et al. (2019), covering the period from pre‑deployment training to post‑rehabilitation support. Vyaltsin et al. (2025), in a literature review, showed that the frequency of stress‑associated disorders in combatants reaches 70%, confirming the scale of the problem and the need for systemic organisational solutions. Karayani and Protsenko (2026) described the phenomenon of chronification of the “combat self” in veterans, whereby identity formed under conditions of constant threat persists after return to civilian life, impeding full resocialisation. Overcoming this phenomenon requires specialised psychotherapeutic interventions aimed at integrating combat experience into a new life perspective. Family involvement, where the wife’s readiness for change correlates with veteran adaptation (r = 0.67), and the creation of positive social expectations, such as the perception of the ‘veteran‑hero’, are crucial components of resocialisation (Shempeleva et al., 2026; Karayani et al., 2025). Methodological approaches by Fettsova et al. (2024) synthesise contemporary strategies for medical‑psychological correction and rehabilitation of combatants. A meta‑analysis by Shahmiri Barzoki et al. (2021) provides an overall PTSD prevalence estimate among combatants of 27.8%, highlighting the systemic nature of the problem. Evdokimov et al. (2023a, 2023b), in bibliometric studies, analysed scientific publication trends, showing a shift from medical aspects to socio‑psychological consequences of combat stress, confirming the relevance of our integrative approach. It is the proactive model, being aimed at preclinical stages, that best aligns with the central finding of this review, namely the key role of subclinical PTSD and cognitive impairments as early targets for prevention.
In summary, the synthesis of the obtained data allows us to formulate six main conclusions. First, combat stress has a dual nature, and the transition to distress is driven by exhaustion of neuroendocrine mechanisms, neuroinflammation, dysbiosis, genetic predisposition, including FKBP5 polymorphisms, and GWAS overlap with schizophrenia and depression, as well as epigenetic changes; however, APOE ε4 is not a moderator of the association between combat stress and PTSD (Wolf et al., 2024; Chepur, 2024; Nievergelt et al., 2019; Reznik, 2022). Second, subclinical PTSD fully mediates the relationship between combat exposure and cognitive errors, justifying mandatory CFQ screening (Price et al., 2024) and serving as the central hub around which the entire system of early diagnosis and prevention should be built. Third, sex differences are critical: resilience is the key protective factor for women, whereas for men partnership and anger control are more important; moreover, social support buffers stress only up to a certain level (Dell et al., 2025; Bridges‑Curry et al., 2025). Fourth, appetitive aggression was found in 58% of retiring soldiers and is associated with harm infliction (aOR = 3.26); alcohol, in turn, partially mediates the link between combat readiness and PTSD (Bigirwa et al., 2025; Baguma et al., 2024). Fifth, effective rehabilitation methods include CBT (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65% in resistant forms), BFB, HHT, iCOVER (knowledge increase by 37%), positive interventions, BTAP (PCL‑5 reduction by 31 points, d = 1.7), Transcendental Meditation (cardiovascular risk reduction by 48%) and folk game practice. Sixth, the proactive multimodal care model, integrating early screening, ‘red zone’ training and family involvement, is significantly more effective than the reactive one (Adler & Gutierrez, 2022b; Karayani et al., 2024), and it should become the organisational foundation for implementing early screening and prevention of subclinical impairments.
Future research directions emerge directly from the identified gaps. Large‑scale multicentre RCTs are needed to evaluate the effectiveness of BTAP, Transcendental Meditation, folk game practice, and the burnout correction programme (Vetrova et al., 2024) with active control groups and long‑term follow‑up (at least 12 months). Longitudinal genetic‑epigenetic studies with repeated biomarker measurements, including cortisol, NPY, IL‑6, and TNF‑α, before, during and after combat deployment, are required to establish causal relationships. Investigation of appetitive aggression and antisocial behaviour in Russian combatant samples using validated instruments, such as the AAS and Patrick’s test, along with analysis of culturally specific factors, is necessary. In‑depth exploration of sex difference mechanisms, encompassing hormonal, neurobiological, and psychosocial aspects, will enable the development of gender‑specific prevention programmes. Validation and adaptation of Russian versions of screening tools, including DES, MIOS, AAS and CFQ, on representative military samples is critically important. The use of wearable devices, such as fitness trackers and pulse oximeters, for continuous monitoring of heart rate variability, sleep quality, and physical activity, with the aim of early detection of allostatic load, is promising. Ecological momentary assessment (EMA) would allow the study of stress dynamics and coping strategies in real combat conditions. Development and testing of proactive multimodal psychological support programmes integrated into combat training and post‑deployment rehabilitation systems, with effectiveness evaluation in quasi‑experimental designs, is needed. Inclusion of combatants’ families in future research is important to assess the role of spousal and social support as a buffer against post‑traumatic stress (Shempeleva et al., 2026). Finally, long‑term consequences of combat stress, covering a period of 5–10 years and including the risk of cardiovascular disease, autoimmune disorders, and accelerated ageing, should be investigated using allostatic load methods (Feigel et al., 2025). Implementation of these directions will enable a transition to personalised prevention and treatment of PTSD in combatants, based on early detection of subclinical cognitive and affective impairments, which constitutes the central finding of this review.
This review has several limitations, including heterogeneity of samples, the small number of RCTs (7 out of 59), predominance of male samples, insufficient genetic data beyond European and African‑American populations, the pilot nature of BTAP, Transcendental Meditation, and folk game practice studies, and the lack of long‑term data for new interventions. Nevertheless, the systematic nature of the review, strict selection criteria, and use of quality assessment tools, in particular JBI, allow the conclusions to be considered reliable and representative for formulating practical recommendations and identifying directions for future research.
This systematic review, synthesising 59 studies with a total participant pool exceeding 18,000 individuals, provides the first comprehensive conceptual framework for understanding the transition from combat stress to pathogenic distress in participants of special military operations. The integration of multi‑level data, from molecular biology to healthcare organization, has identified the central hub of this process: the subclinical level of post‑traumatic stress disorder (PTSD), which fully mediates the relationship between combat exposure and everyday cognitive errors (Price et al., 2024). This phenomenon, previously unexamined in a systematic manner, represents a critical threshold beyond which adaptive responses give way to clinically significant pathology, while simultaneously opening a window for early preventive intervention.
The synthesis of the data obtained demonstrates that the transition from eustress to distress is a multifactorial process involving neuroendocrine mechanisms (hypothalamic–pituitary–adrenal axis exhaustion, elevated cortisol and catecholamine levels), immune dysregulation (neuroinflammation with elevated IL‑1β, IL‑6 and TNF‑α, gut microbiota dysbiosis), genetic predisposition (FKBP5 polymorphisms, overlapping risk loci with schizophrenia and depression) and psychological factors (dissociation, somatisation, moral injury). Notably, the APOE ε4 allele does not moderate the association between combat stress and PTSD, obviating the need for routine testing for this marker (Wolf et al., 2024).
Clinically significant findings demonstrate that dissociation (OR = 6.42) and somatisation (OR = 4.79) represent the strongest independent predictors of severe PTSD, while moral injury, through mechanisms of shame, guilt and entrapment, generates suicidal risk, with dissociation catalysing the transition from suicidal ideation to action (the ‘Ajax effect’ model) (Shabat et al., 2024; Sagalakova et al., 2025). Sex and age differences modulate this process: psychological resilience is the key protective factor for women, whereas partnership and anger control are more important for men; maximal vulnerability occurs at 18–30 years, while after age 50 chronification and treatment resistance increase (Dell et al., 2025; Efremov, 2025). Appetitive aggression, identified in 58% of retiring soldiers, and alcohol as a partial mediator between combat readiness and PTSD expand our understanding of behavioural risks requiring screening (Bigirwa et al., 2025; Baguma et al., 2024).
Practical recommendations arising from this review include mandatory screening using the Cognitive Failures Questionnaire (CFQ) for all military personnel regardless of clinical diagnosis, as well as inclusion of dissociation (DES), moral injury (MIOS), and alcohol screening scales in screening protocols. The diagnostic algorithm should be multi‑level, combining clinical scales (CAPS‑5, PCL‑5), neurophysiological methods (evoked potentials N100, P200, MMN, achieving up to 87% accuracy) and circulating resilience biomarkers (cortisol, NPY, IGF‑1). The rehabilitation strategy should rely on methods with proven effectiveness such as cognitive‑behavioural therapy (SMD = –1.24), EMDR (50–70% remission), VRET (up to 65% in resistant forms), and emerging approaches requiring further investigation in large‑scale RCTs (iCOVER, BTAP, Transcendental Meditation, folk game practice). Organisationally, priority should be given to a proactive multimodal model incorporating early biomarker screening, ‘red zone’ training, integration of psychologists into combat units, gender‑sensitive programmes and active family involvement. It is this model, targeting preclinical stages, that best aligns with the central finding of this review is the critical role of subclinical PTSD and cognitive impairments as early targets for prevention.
Future research should focus on large‑scale multicentre RCTs of novel methods, longitudinal genetic‑epigenetic studies with repeated biomarker measurements before, during, and after combat deployment, investigation of appetitive aggression and antisocial behaviour in Russian samples, validation and adaptation of screening tools, use of wearable devices for continuous allostatic load monitoring, and ecological momentary assessment to study stress dynamics in real combat conditions. Implementation of these directions will enable a transition to personalised prevention and treatment of PTSD in combatants, based on early detection of subclinical impairments.
Competing interests: The authors declare no competing interests in relation to the publication of this manuscript.
Funding: The study was carried out within the framework of the state assignment “Intelligent Systems and Human Abilities” – No. 0138-2026-0016. Registration number in the Unified State Information System for Accounting Research, Development and Technological Work (EGISU NIOTKR): 1023033000550-6-5.1.1.
Acknowledgements: The authors thank reviewers for valuable comments and consultative support during manuscript preparation.
Author Contributions: A. M. Babaev and N. E. Volkova contributed equally to the conceptualisation, data collection and analysis, writing and editing of the manuscript.
AI Usage Statement: Artificial intelligence was used for final text editing of the manuscript to enhance its clarity and literary quality. All scientific statements, data and conclusions are the result of the authors’ independent work.
- Adler, A. B., & Gutierrez, I. A. (2022a). Preparing soldiers to manage acute stress in combat: Acceptability, knowledge and attitudes. Psychiatry, 85(1), 30–37. https://doi.org/10.1080/00332747.2021.2021598
- Adler, A. B., & Gutierrez, I. A. (2022b). Acute stress reaction in combat: Emerging evidence and peer‑based interventions. Current Psychiatry Reports, 24(4), 277–284. https://doi.org/10.1007/s11920-022-01335-2
- Baguma, E. A., Vivalya, B. M. N., Ocen, P. O., & Kasujja, R. (2024). Combat readiness, alcohol abuse, and posttraumatic stress disorder among Uganda peoples’ defence forces soldiers. BMC Psychology, 12(1), Article 581. https://doi.org/10.1186/s40359-024-02068-y
- Barysheva, E. I. (2020). Stress resistance of military personnel in local armed conflict conditions. Penza Psychological Bulletin, 1(14), 50–63. https://doi.org/10.17689/psy-2020.1.5[in Russian]
- Beckner, M. E., Conkright, W. R., Eagle, S. R., Martin, B. J., Sinnott, A. M., La Goy, A. D., & Nindl, B. C. (2021). Impact of simulated military operational stress on executive function relative to trait resilience, aerobic fitness, and neuroendocrine biomarkers. Physiology & Behavior, 236, Article 113413. https://doi.org/10.1016/j.physbeh.2021.113413
- Bigirwa, D. M., Rukundo, G. Z., Muwanguzi, M., Favina, A., & Ashaba, S. (2025). Appetitive aggression and associated factors among military soldiers retiring from active service in Uganda. European Journal of Psychotraumatology, 16(1), Article 2493026. https://doi.org/10.1080/20008066.2025.2493026
- Bridges‑Curry, Z., Meckes, S. J., Fountain, C., Wagner, H. R., Calhoun, P. S., Kimbrel, N. A., Rowland, J. A., Dedert, E. A., Ponzini, G. T., & VA Mid‑Atlantic MIRECC Workgroup. (2025). Combat exposure, social support, and posttraumatic stress: A longitudinal test of the stress‑buffering hypothesis among veterans of the wars in Afghanistan and Iraq. Social Psychiatry and Psychiatric Epidemiology, 60(10), 2495–2504. https://doi.org/10.1007/s00127-025-02864-w
- Bukhtiyarov, I. V., & Glukhov, D. V. (2018). Posttraumatic stress disorder formation in military officers in combat circumstances. Russian Journal of Occupational Health and Industrial Ecology, 2, 10–14. https://doi.org/10.31089/1026-9428-2018-2-10-14[in Russian]
- Campbell, G. M., Biscoe, N., Bonson, A., & Murphy, D. (2026). Association of potential morally injurious events, moral injury and somatic symptoms of health in UK military veterans: A cross‑sectional study. BMC Psychology, 14, Article 56. https://doi.org/10.1186/s40359-025-03788-5
- Chepur, S. V. (2024). Combat stress: Formation mechanisms and targets of directed pharmacological effects. Human Physiology, 50(6), 657–663. https://doi.org/10.1134/S0362119724701123
- Dell, L., Madden, K., Baur, J., Sbisa, A., McFarlane, A., VanHooff, M., Bryant, R., & Lawrence‑Wood, E. (2025). Trauma, resilience and significant relationships: Sex differences in protective factors for military mental health. Australian & New Zealand Journal of Psychiatry, 59(1), 48–59. https://doi.org/10.1177/00048674241286818
- Dudina, E. A., & Blaginin, A. A. (2024). Dynamics of anxiety of combatants during the course of hypobaric hypoxic training. Psychology in Education, 6(2), 210–222. https://doi.org/10.33910/2686-9527-2024-6-2-210-222[in Russian]
- Dvoryanchikov, N. V., Teplova, A. B., & Chernushevich, V. A. (2025). The rehabilitation potential of folklore games in correcting symptoms of avoidance and emotional numbing in combatants. Psychology and Law, 15(4), 20–43. https://doi.org/10.17759/psylaw.2025150001[in Russian]
- Efremov, A. (2026). Age‑specific mental health profiles of combat veterans: Post‑traumatic stress disorder and related disorders. Journal of Rational‑Emotive & Cognitive‑Behavior Therapy, 44, Article 4. https://doi.org/10.1007/s10942-025-00637-7
- Evdokimov, V. I., Shamrey, V. K., & Pluzhnik, M. S. (2023a). Combat stress research prospects in Russian academic publications analyzed using VOSviewer software (2005–2021). Medico‑Biological and Socio‑Psychological Problems of Safety in Emergency Situations, 2, 99–116. https://doi.org/10.25016/2541-7487-2023-0-2-99-116[in Russian]
- Evdokimov V.I., Shamrey V.K., Pluzhnik M.S. Combat stress research prospects in Russian academic publications analyzed using to VOSviewer software (2005–2021). Medicо-Biological and Socio-Psychological Problems of Safety in Emergency Situations. 2023;(2):99-116. (In Russ.) https://doi.org/10.25016/2541-7487-2023-0-2-99-116
- Feigel, E. D., Koltun, K. J., Lovalekar, M., Friedl, K. E., Martin, B. J., & Nindl, B. C. (2025). Advancing the allostatic load model in military training research: From theory to application. Frontiers in Physiology, 16, Article 1638451. https://doi.org/10.3389/fphys.2025.1638451
- Fettsova, L. N., Serova, Yu. S., & Yusupov, V. V. (2024). Methodological approaches to combatants’ medical and psychological correction and rehabilitation. Living Psychology, 11(5), 10–18. https://doi.org/10.58551/24136522_2024_11_5_10[in Russian]
- Goodson, J. T., & Haeffel, G. J. (2022). Treating posttraumatic stress disorder in combat veterans: A guide to using behavior therapy for anxiety and PTSD (BTAP). Clinical Psychology and Special Education, 11(2), 63–80. https://doi.org/10.17759/cpse.2022110204
- Grzesik‑Pietrasiewicz, M., Łach, K., Brożyna, M., Przednowek, K., & Podgórski, R. (2025). The impact of SERE training on selected neurotransmitter secretion in special forces soldiers. Scientific Reports, 15, Article 21853. https://doi.org/10.1038/s41598-025-06270-9
- Kadyrov, R. V., & Venger, V. V. (2021). Complex post‑traumatic stress disorder: Modern approaches to definition of the concept, etiology, diagnostics, and psychotherapy. Psychologist, 4, 45–60. https://doi.org/10.25136/2409-8701.2021.4.35811[in Russian]
- Karayani, A. G. (2024). Combat stress: Problems of definition and classification. Bulletin of the Moscow University of the Ministry of Internal Affairs of Russia, 1, 254–264. https://doi.org/10.24412/2073-0454-2024-1-254-264[in Russian]
- Karayani, A. G., Protsenko, S. A., & Trofimov, N. V. (2025). Social expectations in society as a mechanism for the re‑socialization of combatants. Psychopedagogy in Law Enforcement, 30(4), 378–391. https://doi.org/10.24412/1999-6241-2025-4103-378-391[in Russian]
- Karayani, A. G., & Protsenko, S. A. (2026). “Never returned from the war”: Phenomenon of chronicization of the combat Ego in veterans of combat operations. Extreme Psychology and Personal Safety, 3(1), 210–224. https://doi.org/10.17759/epps.2026030111[in Russian]
- Karayani, Yu. M., Erokhina, A. V., Milcharek, T. P., & Ivanyuk, V. I. (2025). The relationship between the propensity for antisocial behavior and the type of stress response in servicepersons involved in combat operations. Russian Military Psychology Journal, 2(8), 39–45. https://doi.org/10.25629/RMPJ.2025.02.03[in Russian]
- Kasimova, L. N., Kuznetsov, A. N., Kropinova, I. I., Kuznetsov, D. V., Volovik, M. G., Svyatogor, M. V., Sychugov, E. M., Borovskoy, G. Yu., & Khalak, M. E. (2024). Comprehensive assessment of combatants’ psychological and psychophysiological state in exposure therapy of post‑traumatic stress disorder using virtual reality. Modern Technologies in Medicine, 16(5), 35–44. https://doi.org/10.17691/stm2024.16.5.04[in Russian]
- Kuvaeva, I. O., & Volkova, E. V. (2024). Neurochemical markers of coping intelligence. Kazan Medical Journal, 105(2), 260–271. https://doi.org/10.17816/KMJ623568
- Larskikh, S. V., Larskikh, M. V., Mikhan, O. Yu., Potapova, O. N., & Zheleznyakov, M. A. (2023). A study of the effectiveness of interdisciplinary medical care for combatants with PTSD. Medical Psychology in Russia, 15(4), 21–30. [in Russian]
- Liu, Y. Q., Sun, J. L., Jing, M., Liu, G. X., Shi, J., Zhu, X. W., Wang, F., & Ye, M. H. (2024). Effects of positive psychological control intervention on sleep and psychology of officers and soldiers working at sea. World Journal of Psychiatry, 14(10), 1538–1546. https://doi.org/10.5498/wjp.v14.i10.1538
- Lytkin, V. M., Zun, S. A., Kolodin, S. N., & Yatmanov, A. N. (2024). Post‑combat personality changes in combat veterans. Psychology and Psychotechnics, 4. https://doi.org/10.7256/2454-0722.2024.4.69677[in Russian]
- Maslyakov, V. V., Sidelnikov, S. A., Onishchenko, A. N., Barachevskiy, Yu. E., Zakharova, N. B., Verizhnikova, E. V., Shilova, N. A., Fokht, Yu. V., Burekeshev, A. E., & Romanova, I. V. (2025). Hormonal changes and their relation to psychophysiological parameters in combatants. Disaster Medicine, 3, 83–87. https://doi.org/10.33266/2070-1004-2025-3-83-87[in Russian]
- Nievergelt, C. M., Maihofer, A. X., Klengel, T., et al. (2019). International meta‑analysis of PTSD genome‑wide association studies identifies sex‑ and ancestry‑specific genetic risk loci. Nature Communications, 10, Article 4558. https://doi.org/10.1038/s41467-019-12576-w
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo‑Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Pashnin, S. L., Davydova, E. V., & Altman, D. Sh. (2024). Neurocytokine blood profile of veterans of modern combat conflicts with post‑traumatic stress disorder. Russian Journal of Immunology, 27(2), 343–350. https://doi.org/10.46235/1028-7221-16669-NBP[in Russian]
- Pluzhnik, M. S., Evdokimov, V. I., & Shamrey, V. K. (2024). Assessment of mental adaptation disorders for psychological correction tasks in combatants of the special military operation. Bulletin of Psychotherapy, 91, 95–101. https://doi.org/10.25016/2782-652X-2024-0-91-95-101[in Russian]
- Polina, Yu. V., Kuzmina, A. E., & Surikova, A. A. (2026). Psychotherapy methods in the rehabilitation of participants in a special military operation. Universum: Medicine and Pharmacology, 4(133). https://7universum.com/ru/med/archive/item/22396[in Russian]
- Price, M. M., Zanesco, A. P., Denkova, E., & Jha, A. P. (2024). Examining factors associated with self‑reported cognitive functioning in elite military settings: Considerations of combat experiences and post‑traumatic stress symptomology. Scientific Reports, 14, Article 19161. https://doi.org/10.1038/s41598-024-65826-3
- Reznik, A. M. (2022). Overview of research on external factors and genetic predispositions of combat‑related post‑traumatic stress disorder. Bulletin of the Medical Institute of Continuing Education, 4, 46–55. https://doi.org/10.46393/27821714[in Russian]
- Sagalakova, O. A., Truevtsev, D. V., & Zhirnova, O. V. (2025). “The Ajax effect”: The role of moral injury‑related dissociation in the formation of suicidal behavior during combat stress. Psychology and Law, 15(4), 275–297. https://doi.org/10.17759/psylaw.2025150415[in Russian]
- Schneider, R. H., Norris, K. C., & Brook, R. D. (2026). Transcendental meditation to combat psychosocial stress, hypertension and cardiovascular disease. Nature Reviews Cardiology, 23(1), 4–5. https://doi.org/10.1038/s41569-025-01235-x
- Shabat, N., Bechor, U., Yavnai, N., Tatsa‑Laur, L., & Shelef, L. (2024). The link between somatization and dissociation and PTSD severity in veterans who sought help from the IDF combat stress reaction unit. Military Medicine, 189(11–12), e2562–e2572. https://doi.org/10.1093/milmed/usae118
- Shahmiri Barzoki, H., Ebrahimi, M., Khoshdel, A., et al. (2021). Studying the prevalence of PTSD in veterans, combatants and freed soldiers of Iran‑Iraq War: A systematic and meta‑analysis review. Psychology, Health and Medicine, 28(3), 812–818. https://doi.org/10.1080/13548506.2021.1981408
- Shamrey, V. K., Kurasov, E. S., Kolchev, A. I., & Starostina, E. V. (2025). Combat mental pathology: From evolution of views to modern concepts. Russian Journal of Psychiatry, 1, 5–12. [in Russian]
- Shelef, L., Spira, N., Bechor, U., Rotschield, J., & Shadach, E. (2025). The roles of dissociation and depression in PTSD among soldiers exposed to combat. International Journal of Environmental Research and Public Health, 22(6), 814. https://doi.org/10.3390/ijerph22060814
- Shempeleva, N. I., Pestova, I. V., & Trifonova, N. I. (2026). Psychological resources of the family as a condition for adaptation of veterans (participants) of the special military operation. Bulletin of Practical Psychology of Education, 23(1), 61–75. https://doi.org/10.17759/bppe.2026230104[in Russian]
- Soloviev, A. G., Ichitovkina, E. G., Zlokazova, M. V., Davydova, N. E., & Evdokimov, V. I. (2019). Organization of treatment and rehabilitation for combatants with borderline mental disorders. Ekologiya cheloveka (Human Ecology, 26(5), 60-64. doi: 33396/1728-0869-2019-5-60-64
- Telesheva, K. Yu., Savenkova, V. I., Morozova, I. O., Ochneva, A. G., Zeltser, A. I., Andreyuk, D. S., Reznik, A. M., Mukhin, V. N., Melkonyan, G. G., Lytkina, K. A., Mitrofanov, A. A., & Morozova, A. Yu. (2024). Potential neurophysiological markers of combat‑related post‑traumatic stress disorder. Consortium Psychiatricum, 5(2), CP15512. https://doi.org/10.17816/CP1552[in Russian]
- Tseylikman, V. E., Tseylikman, O. B., Feklicheva, I. V., Maslennikova, E. P., Chipeeva, N. A., & Glukhova, V. A. (2018). Psychological, neurobiological and neuroendocrinological features of post‑traumatic stress disorder syndrome. Bulletin of SUSU. Series “Psychology”, 11(4), 73–86. https://doi.org/10.14529/psy180408[in Russian]
- Tuchina, O. P., Sidorova, M. V., Turkin, A. V., Shvayko, D. A., Shalaginova, I. G., & Vakolyuk, I. A. (2018). Molecular mechanisms of initiation and development of neuroinflammation in a model of post‑traumatic stress disorder. Genes and Cells, 13(2), 47–55. [in Russian]
- Ushakov, I. B., Kalmanov, A. S., & Bubeev, Yu. A. (2023). Prospects for the use of xenon‑based special gas mixtures for stress correction in lethal force situations. Medico‑Biological and Socio‑Psychological Problems of Safety in Emergency Situations, 1, 59–67. https://doi.org/10.25016/2541-7487-2023-0-1-59-67[in Russian]
- Van Cutsem, J., van den Berg, N. H., Flores, B., Aïdara, Y., Martin, A., Musat, A., Pattyn, N., & Simonelli, G. (2026). Circulating biomarkers of military‑specific performance resilience: A systematic review. Current Psychiatry Reports, 28(1), 14. https://doi.org/10.1007/s11920-025-01652-2
- Vasilenko, T. D., Petrachevskaya, Yu. L., Smirnov, N. V., & Gulakov, D. A. (2025). Perception of traumatic events by combatants. RSUH Bulletin: Series Psychology. Education, 2, 151–165. https://doi.org/10.28995/2073-6398-2025-2-151-165[in Russian]
- Vasilyeva, A. V., Karavaeva, T. A., Radionov, D. S., & Starunskaya, D. A. (2023). Diagnostic algorithm for post‑traumatic stress disorder. M. Bekhterev Review of Psychiatry and Medical Psychology, 57(1), 83–95. https://doi.org/10.31363/2313-7053-2023-741[in Russian]
- Vetrova, T. V., Leontyev, O. V., Iontsev, V. I., Yakovlev, E. V., & Trokhmanenko, S. V. (2024). The effect of duration of military service on the psycho‑emotional state of military personnel. Bulletin of Psychotherapy, 91, 102–113. https://doi.org/10.25016/2782-652X-2024-0-91-102-113[in Russian]
- Volovik, M. G., Belova, A. N., Kuznetsov, A. N., et al. (2023). Use of virtual reality techniques to rehabilitate military veterans with post‑traumatic stress disorder (review). Modern Technologies in Medicine, 15(1), 74–86. https://doi.org/10.17691/stm2023.15.1.08[in Russian]
- Vyaltsin, S. V., Mirzayeva, M. V., Semenova, N. V., Vdovichenko, O. V., Pyatkin, A. A., & Dvornikov, I. G. (2025). Acute post‑traumatic stress disorder associated with combat stress (literature review). Specialized Healthcare Services, *85*(2), 31–36. https://doi.org/10.56685/18120555_2025_85_2_31[in Russian]
- Wolf, E. J., Miller, M. W., Zhang, R., et al. (2024). No replication of Alzheimer’s disease genetics as a moderator of the association between combat exposure and PTSD risk in 138,592 combat veterans. Nature Mental Health, 2, 553–561. https://doi.org/10.1038/s44220-024-00225-1
- Zaitseva, N. S., & Sizyakina, L. P. (2023). Characteristics of cytokine imbalance in chronic comorbid stress‑induced disorders in combatants in the long‑term follow‑up period. Immunologiya, 44(3), 326–332. https://doi.org/10.33029/0206-4952-2023-44-3-326-332[in Russian]
- Zelenina, N. V., Chernyavsky, E. A., Fedotkina, I. V., Starenchenko, Yu. L., & Yusupov, V. V. (2024). Diagnostics of the level of mental disorders in combatants with acute stress disorder at the stage of hospital rehabilitation. Clinical and Special Psychology, 13(2), 46–60. https://doi.org/10.17759/cpse.2024130203[in Russian]
- Zhilyaev, A. A., & Tipsin, D. V. (2018). The problem of combat stress and rehabilitation of servicemen of the National Guard of the Russian Federation performing service‑combat tasks. Bulletin of the Russian New University. Series: Man in the Modern World, 1, 29–38. https://doi.org/10.25586/RNU.V925X.18.01.P.029[in Russian]
Abstract
References